
Extensor Hallucis Longus Muscle
Table of Contents
Extensor Hallucis Longus Muscle Anatomy
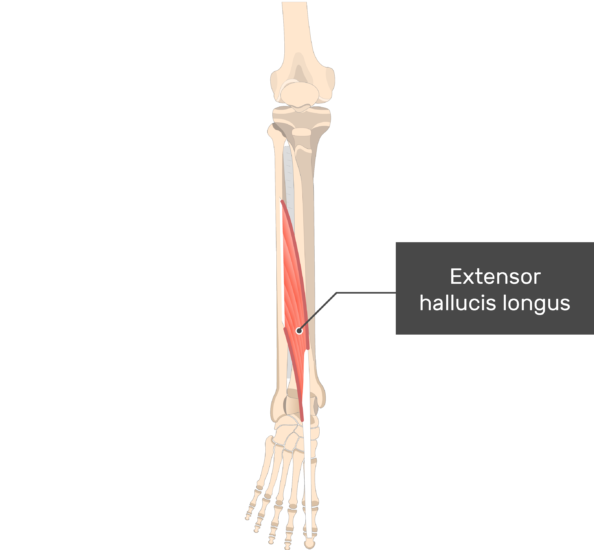
The extensor hallucis longus is a skeletal muscle located in the anterior compartment of the leg. It plays a crucial role in the movement of the foot and toes, specifically in the extension of the big toe.
Extensor hallucis longus muscle is a thin muscle that extends from the middle third of fibula to the distal phalanx of the big toe (hallux).
The muscle belongs to the anterior compartment of the leg together with three other muscles; extensor digitorum longus, tibialis anterior, and fibularis tertius muscles.
Specifically, the extensor hallucis longus inverts the foot, dorsiflexes the foot at the ankle, and stretches the hallux. Numerous conditions can affect the extensor hallucis longus muscle, such as anterior compartment syndrome, tendinitis, tendon rupture, and nerve damage that results in foot drop.
Origin
Middle third of medial surface of fibula, interosseous membrane
Insertion
Base of distal phalanx of the great toe
Nerve supply
Extensor hallucis longus is innervated by the deep fibular nerve (root value L5 and S1).
Blood supply
The blood supply for extensor hallucis longus mainly comes from the anterior tibial artery and its branches. In addition, the muscle can be supplied by the branches of fibular artery.
Lymphatic Drainage
There are two main categories of lymphatic vessels in the lower limb: superficial and deep channels. The superficial lymph veins in the lower leg are further subdivided into two groups: the lateral group follows the small saphenous vein, while the medial group follows the bigger saphenous vein.
Deep lymph vessels that trace the path of the corresponding arteries and veins include the peroneal, posterior, and anterior tibial vessels. The popliteal, superficial inguinal, deep inguinal, external iliac, lumbar, or aortic lymph nodes are the lymph nodes that receive drainage from the lower limb lymph veins.
Actions
extensor hallucis longus muscle is the extension of the big toe (hallux). This action happens in both metatarsophalangeal and interphalangeal joints of hallux.
Structure and Function
The anterior side of the fibula is the source of the extensor hallucis longus, which inserts at the base and dorsal center of the distal phalanx of the hallux. It runs inferiorly and medially to its insertion site at the base of the great toe’s distal phalanx. It is located on the anterior side of the lower leg, between the tibialis anterior and extensor digitorum longus muscles. Between the extensor hallucis longus and the tibialis anterior muscles are the anterior tibial artery, vein, and deep peroneal nerve.
In order to keep the muscle from bowstringing or subluxing, the extensor hallucis longus muscle fibers go inferiorly and medially before terminating in a tendon that passes beneath the inferior extensor retinaculum.
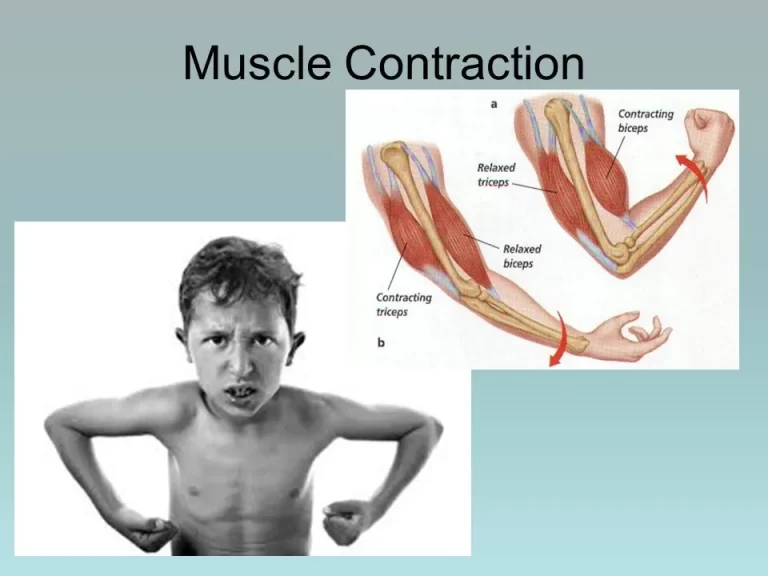
The extensor hallucis longus is primarily responsible for dorsiflexing the foot at the ankle and extending the hallux. Muscle contraction causes the foot and big toe to rise toward the shin (dorsiflexion) because it originates on the fibula, the lateral bone of the anterior leg, and ends on the tendon of the distal phalanx of the hallux.
This motion permits the foot to be cleared off the ground during the swing phase, which is essential to gait. Consequently, foot drop—a lack of dorsiflexion—and a distinctive high-stepping gait can be caused by injury or degeneration of the muscles or deep peroneal nerve, which innervates the anterior compartment.
Because it inserts on the distal phalanx of the hallux, the most medial toe, the extensor hallucis longus contributes to weakly inverting the foot in addition to extending the hallux and dorsiflexing the foot at the ankle. Because the tibialis anterior has a strong action in inverting the foot, loss of the extensor hallucis longus can also cause weakness in foot inversion, but this is usually not clinically significant.
Embryology
About five weeks after conception, the embryo starts to produce its limb buds. The mesoderm migrates into the limb bud and forms an anterior and posterior condensation, which eventually forms the skeletal and muscular components of the lower limb.
The lower limb’s flexor and adductor muscles will form from the anterior condensation, while the lower limb’s extensor and abductor muscles will originate from the posterior condensation.
The creation of limb bud musculature is influenced by several variables, including as HOX genes, retinoic acid, sonic hedgehog (SHH), apical ectodermal ridge (AER), and the zone of polarizing activity (ZPA). The global organizing gradient known as retinoic acid triggers the synthesis of transcription factors that determine limb polarization and regional differentiation. By inducing mitosis, the apical ectodermal ridge (AER) generates fibroblast growth factor (Fgf), which encourages the expansion of the limb buds.
Tbx4 stimulates Fgf10, a particular fibroblast growth factor important in hindlimb development. The zone of polarizing activity (ZPA), which encourages the formation of the limb bud along the anterior-posterior axis, is responsible for producing SHH. Certain HOX genes, including Hoxd-9, Hoxd-10, Hoxd-11, Hoxd-12, and Hoxd-13, which are crucial for limb polarization and regional determination, are activated by SHH. In the human embryo, these genes regulate patterning and, as a result, the shape of the developing limb. Leg deformities may result from mistakes in the expression of the Hox gene.
Anatomical Variantions
The base of the big toe’s distal phalanx is where the extensor hallucis longus muscle enters. There are, however, a number of variations that could have one or more additional tendinous slips that attach into nearby bones or tendons. The extensor hallucis longus muscle can be employed in tendon transfer procedures to treat disorders including hallux varus, talipes equinovarus, and clawed hallux coupled with a cavus foot, which makes these physiologic variations clinically noteworthy.
The following are the three most typical insertion patterns:
- Pattern 1 (65%): Single tendinous insertion on the dorsal side of the base of the big toe’s distal phalanx.
- Pattern 2 (26.7%): two tendons where the muscle tendon ends
- Pattern 3 (8.3%): Muscle terminated in three tendinous slips
To avoid adverse surgical outcomes during tendon transfer procedures, radiologists and surgeons must be aware of the extensor hallucis variations.
Strengthening exercise
Clinical relevance
The compartment syndrome which is a relatively common cause of the dysfunction of the extensor hallucis longus muscle. The compartment syndrome is a medical emergency caused usually by blunt force trauma to the anterior aspect of the leg. Due to strong and inflexible fascial membranes, the swelling increases the pressure which compromises the circulation and function of the muscles (e.g. the extensor hallucis longus) within that space.
The big toe’s extension and the foot’s dorsiflexion at the ankle are both facilitated by the extensor hallucis longus. This is why the range of motion and motor strength of the ankle and big toe are assessed during the physical examination. Reduced or nonexistent motor strength may be a sign of L5 nerve root weakening or injury to the extensor hallucis longus and anterior compartment muscles of the leg.
Tendonitis and rupture can also be related to the extensor hallucis longus. Most of the extensor hallucis longus tendon injuries that have been reported in the literature have been caused by lacerations. Nonetheless, at least one documented instance of an atraumatic extensor hallucis longus tendon tear in a patient without antecedent medical issues has been documented in the literature. Tendonitis, which is caused by an overstressed tendon that causes discomfort and inflammation, can also affect the extensor hallucis longus tendon.
The most frequent causes of tendonitis in the lower limb’s extensor muscles include falling arches in the feet, overexertion during exercise, and excessive calf muscle tension. Stretching and NSAIDs can be used to treat mild instances of extensor tendonitis. In addition to NSAIDs and stretching, a walking boot may be utilized in more serious instances.
Damage to the deep peroneal nerve is another frequent lesion to the anterior compartment of the lower leg. In this scenario, the patient’s incapacity to extend their toes and dorsiflex their foot at the ankle would be evident. A profound peroneal nerve injury can have a significant effect on gait, causing a recognizable high-stepping stride to make up for the foot drop.
Surgical Considerations
Ruptures or other unusual injuries can occur to the extensor hallucis longus tendon. The patient may present with a dropped hallux and loss of dorsiflexion in the event of a rupture or significant damage, which may impair gait. This can be surgically repaired by transferring the first slip of the extensor digitorum longus and extensor hallucis brevis to the damaged extensor hallucis longus. In tendon transfer surgery, the extensor hallucis longus tendon itself can be utilized to treat disorders like talipes equinovarus and hallux varus.
Ruptures or other unusual injuries can occur to the extensor hallucis longus tendon. The patient may present with a dropped hallux and loss of dorsiflexion in the event of a rupture or significant damage, which may impair gait. This can be surgically repaired by transferring the first slip of the extensor digitorum longus and extensor hallucis brevis to the damaged extensor hallucis longus. In tendon transfer surgery, the extensor hallucis longus tendon itself can be utilized to treat disorders like talipes equinovarus and hallux varus.
Treatment and prevention of ischemia and necrosis of the neurovascular structures and muscles depend on the identification of compartment syndrome. Anterior compartment syndrome patients frequently exhibit discomfort that is excessive for the clinical circumstances. Ankle stiffness, pain while passively stretching the affected muscles (the most sensitive test result prior to the development of ischemia), and pain when palpating the affected muscles are common physical exam findings of anterior compartment syndrome.
Since the venous system is largely affected by compartment syndrome, arterial pulses are often unharmed. Dorsiflexion weakness is another relevant sign for anterior compartment syndrome. Measuring compartmental pressures is necessary for the final diagnosis of anterior compartment syndrome. The diagnosis of compartment syndrome is verified by a resting compartment pressure of more than 30 mm Hg. Time is critical in cases of acute compartment syndrome; full recovery is expected if treatment is received within 6 hours of ischemia, but necrosis develops after 6 hours. A subcutaneous fasciotomy is the definitive treatment for acute anterior compartment syndrome.
FAQ
In the anterior compartment of the lower leg, the slender Extensor hallucis longus (EHL) muscle is located between the Tibialis anterior and the Extensor Digitorum Longus. It supplies the metatarsophalangeal joint with its major active extension force and the interphalangeal joint with its solitary active extension force.
The tibialis anterior muscle works in combination with the hallucis longus muscle.
Extensor digitorum longus, Tibialis anterior, and Peroneus tertius work as a Synergist.
Antagonists include Tibialis posterior, Soleus, Plantaris, Peroneus longus and brevis, Gastrocnemius, Flexor digitorum longus, and Flexor hallucis longus.
One muscle located in the leg’s anterior compartment is the extensor hallucis longus. Its tendon arises from between the tibialis anterior and extensor digitorum longus muscles to enter into the big toe, and it is situated deep in these muscles.
Extensor hallucis The tendons of the extensor muscles longus and extensor digitorum longus, which run along the front of the ankle and foot, pull the toes back up (extension). If these muscles are overused or too tight, they can produce inflammation and pain at the front of the ankle, particularly when flexing the joint.
Foot weakness is rarely caused by injuries to the extensor hallucis longus. Usually resulting from trauma, they are characterized as open lacerations or closed ruptures based on the mode of damage; the latter is quite uncommon. They are frequently seen in the distal tendon.

One Comment