
Superior Oblique Muscle
Table of Contents
Superior Oblique Muscle Anatomy
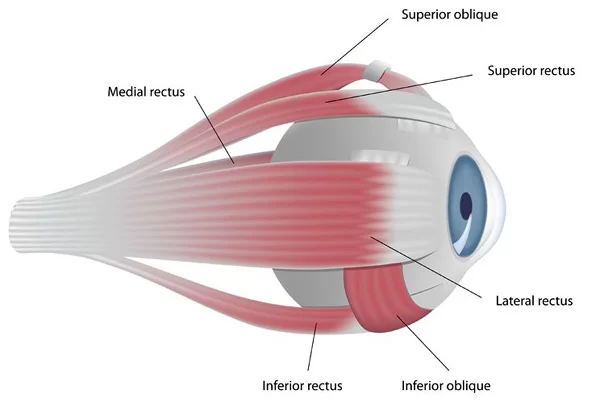
- The superior oblique muscle is one of the six extraocular muscles that control eye movements.
- The superior oblique muscle is the longest muscle in this group, spanning from the body of the sphenoid bone to the superolateral aspect of the eyeball.
- The superior oblique muscle is fusiform and it originates in the upper, medial side of the orbit (i.e. from beside the nose) which abducts, depresses, and internally rotates the eye.
- It is the only extraocular muscle innervated by the trochlear nerve (the fourth cranial nerve).
Origin
- The superior oblique muscle originates from the body of the sphenoid bone, medial to the origin of the levator palpebrae superioris muscle, and superomedial to the optic canal.
Insertion
- This muscle insertion is located behind the equator of the eyeball, between the attachments of the superior rectus and lateral rectus muscle.
Nerve supply
- The superior oblique muscle is the only extraocular muscle that receives its innervation through the trochlear nerve (CN IV).
Blood Supply
- Superior oblique muscle supply by small branches of the anterior ciliary arteries which are derived from the ophthalmic artery.
- The lateral muscular branch of the ophthalmic artery provides the circulatory supply for the superior oblique muscle. This branch also supplies blood to the levator palpebrae superioris muscle, and the lateral and superior rectus muscles. The medial muscular branch, which provides blood to the remaining extraocular muscles, is another branch that the ophthalmic artery splits into.
- The superior oblique muscle’s venous drainage resembles that of the other extraocular muscles. The superior and inferior orbital veins receive deoxygenated blood from the muscles after it has passed through the four vortex veins that originate from the posterior side of the eye. The cavernous sinus is the final destination of the orbital veins, sometimes referred to as the ophthalmic veins.
Actions
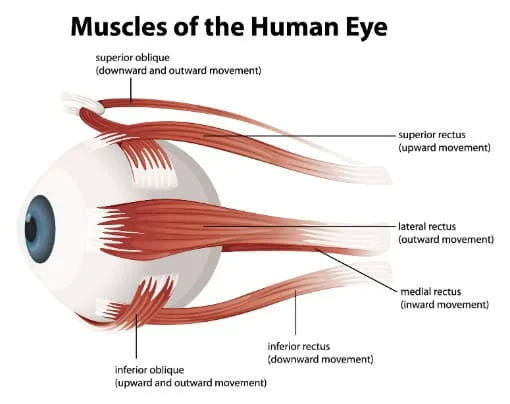
- When the eyeball is in a neutral position, the superior oblique muscle is responsible for abduction (directed laterally from the nose), depression (inferiorly), and internal rotation (movement of the superior pole of the eye medially) of the eyeball.
Relations:
- The superior oblique muscle is situated in the upper medial portion of the orbit and it is adjacent to its medial wall.
- The muscle is located superior to the medial rectus and medial to both the superior rectus and levator palpebrae superioris muscles.
Assessment
Clinical evaluation of all the extraocular muscles is often performed by having the patient track the clinician’s finger in the air in the shape of an “H.” The superior oblique muscle can be isolatedly tested by having the patient glance inward and downward.
Even though the movement of the eye in a down-and-out direction is the particular function of the superior oblique, the lateral rectus and inferior rectus might contribute to this movement, making it difficult to separate the superior oblique’s function by having the patient stare in this direction. Rather, the patient looks down and in to test the superior oblique, as was previously described.
One may isolate the activity of the superior oblique by contracting the medial rectus, which cancels out the action of the inferior rectus muscle.
Embryology
When compared to the other extraocular muscles, the development of the superior oblique muscle is not special. That being said, these extraocular muscles differ from periocular tissues in that, unlike their connective tissue tendons, they originate from paraxial mesoderm in the prechordal plate. While the majority of other extraocular muscles emerge during week five of development, the superior oblique muscle and the medial rectus do so at week six.
The specific growth of the muscle is responsible for the distinct pulley action of the superior oblique along the trochlea. Studies on embryology demonstrate that throughout the initial stages of development, the cartilaginous pulley, the insertion tendon, and the muscle itself move in a straight path. The pulley motion is produced when the tendon starts to wrap around the trochlear cartilage, which happens at about 12 weeks.
Physiologic Variantions
There are physiological differences across people when talking about certain measures of the superior oblique muscle. Individual differences may exist in some measures, including muscle size, tendon length, insertion point, and angle at which the muscle approaches the trochlea.
Additionally, as was previously mentioned, when comparing people, the superior temporal vortex vein takes a different route with respect to the superior oblique muscle, either going through or around the muscle.
Clinical relations:
The disorder known as strabismus, which can manifest as acquired paralytic strabismus in children, is typically caused by ocular misalignment as a result of malfunctioning CN III, IV, or VI. When there is a specific CN IV dysfunction, the superior oblique muscle becomes paralyzed.
This causes hypertropia, which is an upward deviation of the eye caused by the superior rectus muscle acting without resistance, commonly during contralateral gazing. For instance, when gazing to the left, a patient with right CN IV palsy may have right hypertrophia. The misalignment of the eyes may be corrected by strabismus surgery. Muscle relocation, tightening, or loosening are surgical alternatives.
Superior Oblique Palsy
One potential ailment that might be caused by injury to CN IV is superior oblique palsy. Trauma, tumors, and vasculopathy can all harm CN IV. A typical symptom of this palsy is difficulties looking down. As a result, a patient may complain of difficulties going down stairs or turning pages in a book.
Patients who stare downhill or to the other side may complain of verticle diplopia. Reversing the head’s angle might potentially reduce the appearance of double vision. Double vision is worse when the head is tilted to the affected side.
- The superior oblique muscle functions are impaired usually caused by lesions of the trochlear nerve somewhere on its long path from the brainstem to the orbit.
- The Isolated injury of this nerve is fairly rare, but it’s usually combined with injuries of other cranial nerves.
- The main symptom of superior oblique dysfunction is diplopia (double vision) which occurs when directing the gaze downward Diplopia occurs because this muscle functions as a depressor of the eyeball, especially when the eye is in an abducted position.
Etiology:
- Most children with fourth nerve palsy are affected by birth and The child may have other health problems along with congenital fourth nerve palsy.
- In adults, the most common cause of fourth nerve palsy is injury. The injury can occur that causes whiplash or concussions. Another common cause is poor blood flow related to diabetes.
= Less common causes of fourth nerve palsy include:-
- A vascular disease that happens with diabetes. This can decrease the blood supply to the nerve.
- A bulging area of an artery (aneurysm). This can press on the nerve or burst and decrease the blood supply to the nerve.
- Increase in pressure inside the skull (increased intracranial pressure). This can press on the nerve.
- Infection
Symptoms:
- Double vision (diplopia) is a common symptom of fourth nerve palsy.
- One iris is higher than the other. The iris is the colored part of your eye.
- Holding your head at a tilt. This is to help with the vision problem.
- Pain, usually above the eyebrow. This can happen if the fourth nerve palsy is idiopathic or related to diabetes.
Treatment:
- The treatment of fourth nerve palsy includes both non-surgical and surgical interventions.
- Many cases of acute acquired fourth nerve palsy spontaneously resolve with time.
- Observation
- Prism therapy
- Occlusion
- Botulinum toxin injection
- Strabismus surgery
FAQ
These muscles are distinct in that they connect to the posterior portion of the eyeball, have an angular attachment to the eyeball, and do not arise from the common tendinous ring. The purpose of the superior oblique is specifically to turn the eye and shift it downward and outward.
In addition to aiding in trunk rotation, the external obliques on either side carry out a number of other essential tasks. These muscles aid in the overall downward pull of the chest, which constricts the abdominal cavity. The external oblique muscle aids in the rotation of the spine, despite its relatively small size.
Choose a comfortable spot to sit or stand. Without moving your head, draw an unseen figure 8 eight to ten feet in front of you on the floor. After tracing the lines in one way, turn around and trace the opposite direction. Every day, do three to five sets of the workout.
Failure of the eye’s maximum adduction is caused by weakness in the superior oblique muscle. As a result, there is vertical diplopia, with the largest image separation happening while looking down and away from the affected side (adduction).
The superior oblique and inferior obliques are the two oblique muscles. They don’t come from the same tendinous ring as the recti group of muscles. Unlike the recti muscles, which approach the eyeball straight, the oblique muscles approach it angularly from their origin.

2 Comments