
Deltoid Muscle
Table of Contents
Introduction
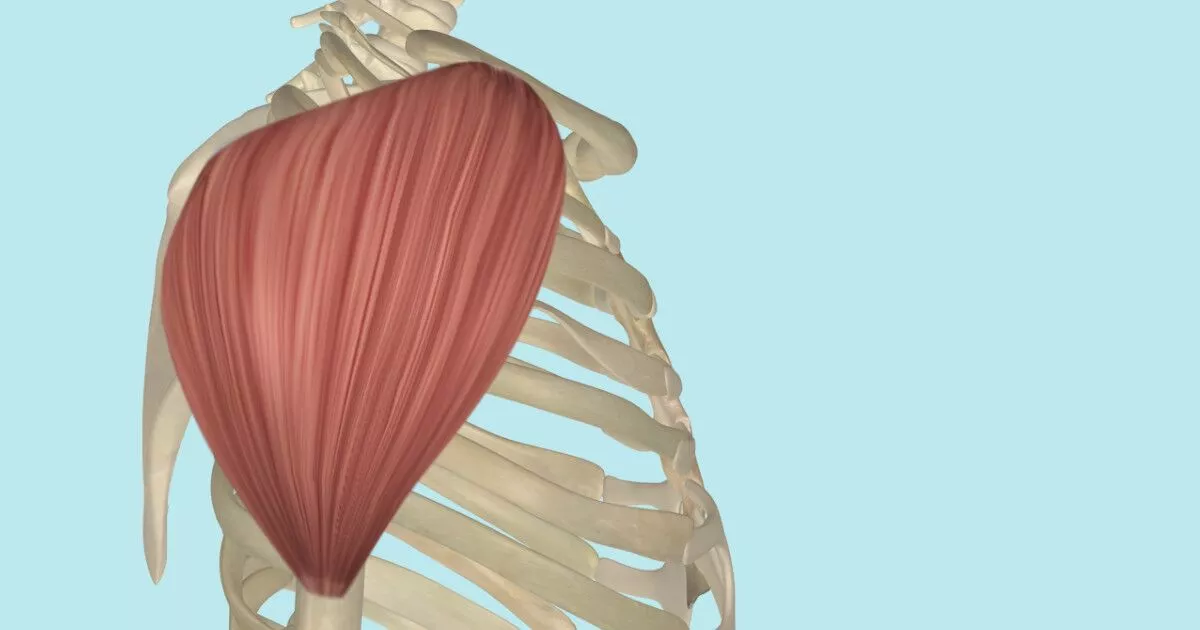
The Deltoid muscle is a large triangular-shaped muscle that lies over the shoulder joint and it gives the shoulder its rounded contour.
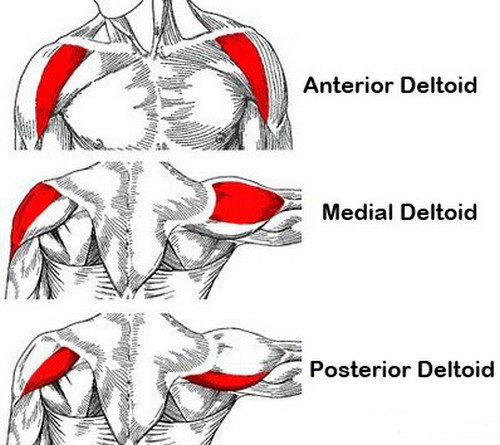
Deltoid muscle contains three-part
- anterior or clavicular,
- middle or acromial, and
- posterior or spinal
Deltoid muscles act as an abductor of the shoulder and stabilizers of the humeral head. as well as assist in elevation forward.
The deltoid is a very powerful muscle and is used in many ADLs and many athletic activities.
Origin of Deltoid muscle:
The Deltoid muscle originates from the anterior border and the adjoining surface of the lateral one-third of the clavicle,
the lateral border of the acromion process where four septa of origin are attached and the lower lip of the crest of the spine of the scapula.
Insertion of Deltoid muscle:
The Deltoid muscle is inserted on the deltoid tuberosity of the humerus.
Nerve supply of Deltoid muscle:
The nerve supply of The Deltoid muscle is the Axillary nerve (C5, C6).
Blood supply of Deltoid muscle:
The blood supply of the deltoid muscle is the thoracoacromial artery (acromial and deltoid branches), the circumflex humeral arteries, and the profunda brachii artery.
Lymphatic Drainage
The deltopectoral lymph nodes, which are situated inside the deltopectoral groove next to the cephalic vein, are responsible for the lymphatic drainage of the deltoid.
The action of Deltoid muscle:
The multipennate acromial fibres are powerful abductors of the upper limb at the shoulder joint from beginning to 90 degrees.
A multipennate arrangement allows a large number of muscle fibres to be packed into a small volume. As the strength of contraction of a muscle is proportional to the number of muscle fibres present in it (and not on their length), a multipennate muscle is stronger than other muscles having the same volume.
The anterior fibres are flexors and Internal rotators of the shoulder.
The posterior fibres are extensors and external rotators of the shoulder.
Structures under Cover of the Deltoid Muscle
Bones
i. The upper end of the humerus.
ii. The coracoid process.
Muscles
Insertions of
i. Pectoralis minor (on the coracoid process).
ii. Supraspinatus, infraspinatus, and teres minor inserted on the greater tubercle of the humerus.
iii. Subscapularis (on the lesser tubercle of the humerus).
iv. Pectoralis major, teres major, and latissimus dorsi inserted on the intertubercular sulcus of the humerus.
Origin of
i. Coracobrachialis and short head of biceps brachii muscle from the coracoid process.
ii. Long head of the biceps brachii muscle from the supraglenoid tubercle.
iii. Long head of the triceps brachii muscle from the infraglenoid tubercle.
iv. The lateral head of the triceps brachii muscle from the upper part of the posterior surface of the humerus.
Vessels
i. Anterior circumflex humeral.
ii. Posterior circumflex humeral
Nerve
Axillary nerve.
Joints and ligaments
i. The musculotendinous cuff of the shoulder.
ii. Coracoacromial ligament.
Bursae
All bursae around the shoulder joint, including the subacromial or subdeltoid bursa
Associated Muscles
The teres minor, subscapularis, supraspinatus, and infraspinatus are among the muscles that contract with the deltoid. When the deltoid works to abduct past 15 degrees, these muscles stabilize the glenohumeral joint and aid in initial abduction from 0 to 15 degrees.
Embryology
The segmented paraxial mesoderm is the source of all striated muscles in the trunk and limbs, including the deltoid muscle. Somata are the bilaterally paired blocks into which the paraxial mesoderm separates. Myogenic precursors (myoblasts) in the somites move toward growing limb buds during the 5th week of development. In the dorsal and ventral limb buds, these myoblasts condense into two primary groups: dorsal and ventral muscle mass. The dorsal muscular mass gives rise to the deltoid muscle.
Anatomical Variations
Anatomical variations of the deltoid have been documented in the literature, regardless of their rarity. There have been multiple case reports describing distinct facial sheaths on the posterior aspect of the deltoid. The posterior deltoid fibers were completely separated from the remainder of the muscle, according to one case report. These variations should be recognized since they could cause confusion when posterior deltoid flap procedures are being performed. Because of its unique fascia and position, the surgeon can mistake this variety for the teres minor.
Anomalies include aberrant insertion into the humerus’s medial epicondyle, among other observed anatomical abnormalities. The brachial artery, ulnar nerve, and median nerve are superficially reached by the fibers where they are inserted. Surgeons should therefore be aware of the neurovascular proximities and exercise caution if this variation is evident. Deltoid strap abnormalities have also been documented in the literature. These straps pass through the posterior deltoid fibers perpendicularly. Additionally, because they can be mistaken for ordinary muscle fibers, surgeons need to be aware of abnormal muscles.
There are numerous reports of thoracoacromial artery variations in the literature. As mentioned earlier, the thoracoacromial artery nourishes the deltoid muscle by passing through the cephalic vein’s deltopectoral groove. Two kinds of differences have been identified. In type I, it enters the deltoid muscle through a tunnel that crosses the interval. In type II, it follows the cephalic vein and spans the gap. But after that, it will curve back in the direction of the pectoralis major.
Clinical importance
The most common abnormalities affecting the deltoid muscle are tears, fatty atrophy, and enthesopathy. Deltoid muscle tears are unusual and commonly related to traumatic shoulder joint dislocation or massive rotator cuff injury. Muscle atrophy may result from various causes like ageing, disuse, denervation, muscular dystrophy, cachexia, and iatrogenic injury.
Deltoideal humeral enthesopathy is an exceedingly rare condition that is related to mechanical stress. Conversely, deltoideal acromial enthesopathy is likely a hallmark of seronegative spondyloarthropathies and its detection should probably be followed by pertinent clinical investigation and serological investigation.
The incapacity to abduct the arm does not necessarily signify a deltoid malfunction. Impaired arm abduction is a symptom of proximal neuromuscular diseases. One example of a neurological issue is Lambert Eaton disease. Polymyositis/dermatomyositis, polymyalgia rheumatica (stiffness instead of weakness), and maybe aluminum hydroxide-containing vaccination adverse effects are examples of muscular inflammatory processes.
All of these disorders may manifest as weakness in the proximal muscles or as an incapacity to abduct the arm. Patients with deltoid weakness may also have malnourishment or cachexia from chronic illness as differential diagnosis. Upon noticing that the patient is unable to abduct the upper limb, all clinicians keep these differentials in mind.
Deltoid muscle exercise
Exercise for Deltoid is the best way to make your shoulder powerful and flexible to perform all day-to-day activities with ease.
Mainly 2 types of Deltoid muscle exercise
- Deltoid muscle-strengthening exercise
- Deltoid muscle stretching exercise
Stretching exercise of the deltoid muscle
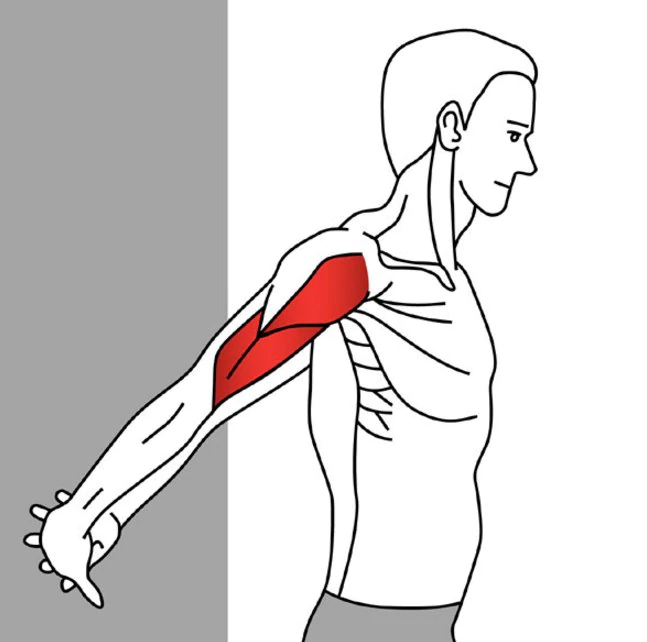
Anterior deltoid muscle stretching exercise
You have to do behind-the-back stretches to open up the front of your shoulder. Stand with your feet apart about hip-width, shoulders are relaxed so that your shoulder blades are tucked down along either side of your spine. Clasp your hands behind your lower back, then lift them away from your body while keeping your elbows straight. Lift until you feel a stretch, then hold the stretch for 30 seconds.
Stay upright while doing this stretch and resist the urge to bend forward.
If you have difficulty clasping your hands behind your back, hold a towel between your hands.
Do this stretch 3 times.
Lateral deltoid muscle stretching exercise
Start with the basic side deltoid stretch. Stand with your feet apart about hip-width and position one arm across your chest with your elbow bent slightly. Grasp just your upper arm above your elbow with your other hand and push your elbow towards your chest. Hold the stretch for 30 seconds, then repeat with the other arm.
gently push your arm until you feel a stretch. your shoulders should be relaxed with your shoulder blades tucked alongside either side of your spine.
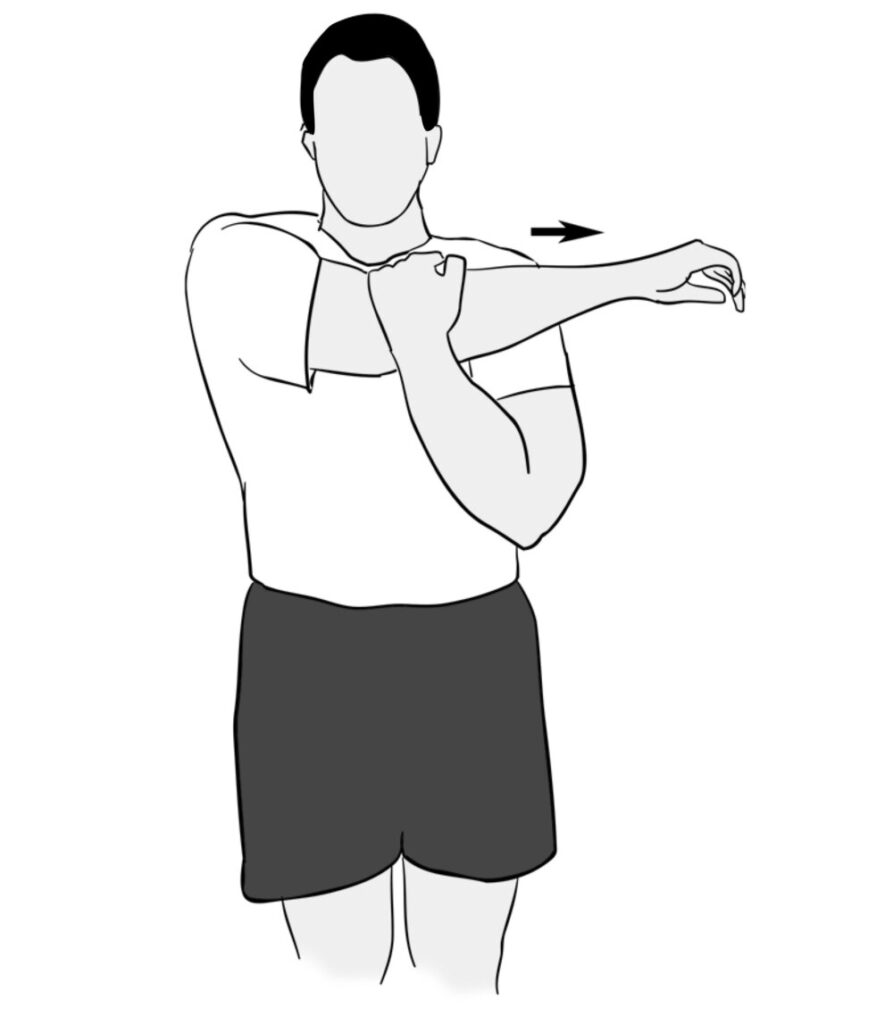
Posterior deltoid muscle stretching exercise
Posterior deltoid Start with crossover arm stretches. Relax your shoulders, pulling them back so that your shoulder blades fall down along either side of your spine. Reach one arm across your body and grip the upper arm with your other hand. Gently pull it as far as possible across your chest until you feel a stretch at the back of your shoulder. Hold for 30 seconds. Repeat the stretch with the other side.
Be sure to grab your upper arm, not your elbow joint.
Strengthening Exercise of the deltoid muscle
Static Deltoid Contraction
deltoid strengthening exercise begins with standing next to a wall with your back and elbow straight. Gently push your arm to the side against the wall as hard as possible and comfortably without any problem. Hold for 5 seconds and repeat 10 times on each side without pain.

Resistance Band Forward Raises
This exercise begins with standing with your back straight and holding a resistance band. Slowly raise your arm to your shoulder level, keeping your arm and back straight. Then slowly lower back down. Perform 10 repetitions of 3 sets without pain.

Anterior deltoid raise
For this exercise, you have to stand with your feet apart about hip-width and grab a dumbbell in both hands with your arms by your sides.
Your elbow should be straight, slowly lift the dumbbell directly in front of you to a height of shoulder with your palms facing each other.
Slowly Lower back down to the initial position and then repeat.
Do 10 repetitions of 3 sets.

Callahan Press
This exercise is useful for all three heads of the deltoids.
For this exercise, you have to stand with feet apart about hip-width apart, and hold a dumbbell in both hands.
Raise your arms out to your sides with your elbows flexed 90 degrees.
Your upper arms should be the same in line with your shoulder joint, and your hands should point toward the ceiling. This is the starting position.
Move your forearms in front of you and then turn your palms inside toward your face.
Then reverse your movement to return to the starting position.
Press the weights directly above your shoulders, and then reverse your movement to return to the starting position.
Do 10 repetitions of 3 sets.
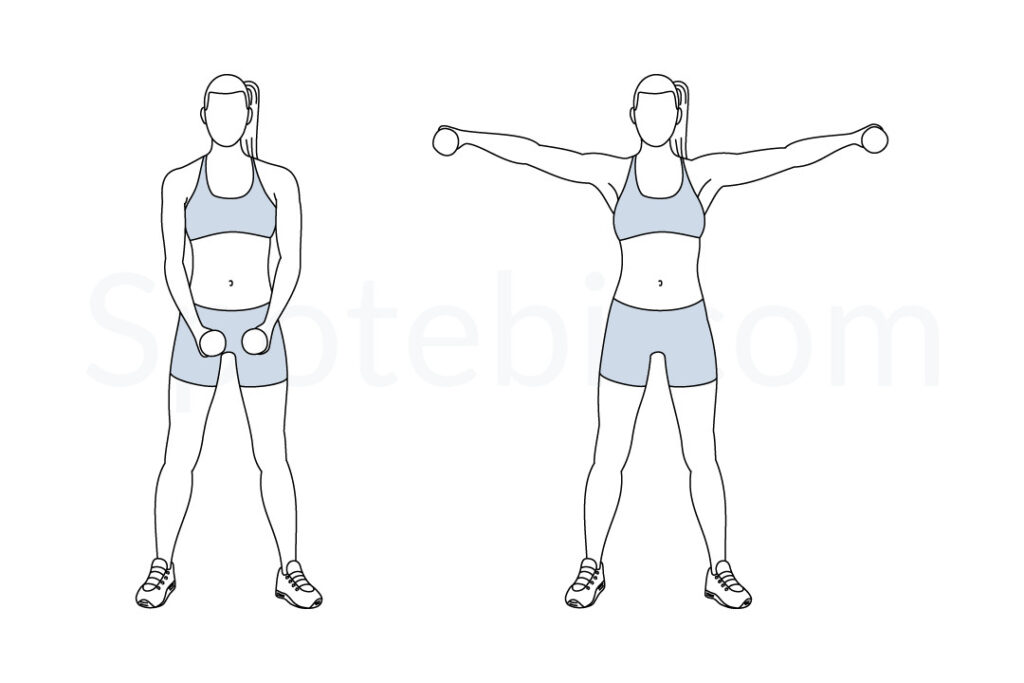
Dumbbell Lateral Raise
This is a very effective strengthening exercise that targets the anterior and the medial part of the deltoid muscles. Additionally, the exercise also targets the upper back, trapezius, and core.
For this exercise, you have to stand with feet apart about hip-width apart. hold dumbbells in both hands with a pronated grip.
Slowly raise your arms in an arc to the sides until the dumbbells are in line with your shoulders. your elbows should be straight and ensure that the arms are parallel to the ground.
hold for some time and return to the starting position.
Do 10 repetitions of 3 sets.
5 Comments