

ABOVE KNEE AMPUTATION: Indication, Exercise, Prosthesis
The above-knee amputation is the most common type of amputation performed in the femur. The above-knee amputation is a lengthwise amputation of the femur just above the knee. It is often performed to remove part of the femur for a malignant tumor or to prevent the spread of cancer or Infection. The above-knee amputation is a mutilating procedure and it requires a long recovery period.
Table of Contents
Defination of Amputation:
- Amputation is defined as the Removal of limbs partly or totally from the body.
Indication Of Above Knee Amputation:
- Malignant tumors
- Nerve injuries and infection
- Extreme heat and cold
- Peripheral Vascular Insufficiency
- Congenital absence of limbs or malformations
- severe infections like gas gangrene,
- osteomyelitis
- Trauma
Levels Of Amputation:
Level Of Amputation In Above Knee
- Hemipelvectomy
- Hip Disarticulation
- Transfemoral (Above Knee Amputation)
- Knee Disarticulation
Above Knee Amputation Treatment
- The Optimal Length of the above knee Amputation is 23 to 30 cm as measured from the tip of the greater trochanter. The minimal length for a useful stump is 7.5cm.
Before Surgery
- Before your surgery, your physical therapist may Prescribe exercises according to your preoperative conditions, and to improve the flexibility and strength of the hip and knee. Physiotherapists teach you how to walk with an assistive device like a walker or crutches. Educate you about the procedure.
Preoperative Training Programm
- Prevent the formation of thrombosis by maintaining the circulation by movement of limbs.
- Prevention of chest complications by deep breathing, coughing, and postural drainage preserves mobility of all joints
- Improve mobility of other areas like trunk, pelvis, shoulder girdle
- Teach how to position the limb in bed Teach the patients how to transfer, monitor of wheelchair, single-leg standing, and balance
- in the recovery from amputation, Psychological reassurance plays an important role.
Early postoperative stage
- To check the efficacy of Preoperative training
- Prevent chest complications and thrombosis
- Prevention of contracture and deformities:
- the common contracture is knee flexion contracture. contracture is prevented by the proper positioning of an amputated limb.
- Maintenance of strength and mobility
- The patient can be motivated to move in the bed by pushing up the body on the arms. This push-up exercise has the advantage of strengthening the muscles in the upper limb which is necessary for using assistive devices later on. strengthening exercise should be given to the whole body except joint proximal to above knee amputation.
- Bed activities like bridging, and rolling can be useful to start bed mobility.
- Active assisted and self-resist exercise can be initiated after 3-4 days of surgery. Assisted hip flexion, extension, abduction, and adduction movements can be performed. Isometric exercise was also initiated.
Management of the stump:
- Improper management of stumps is one of the common causes of delayed rehabilitation. Surgical trauma is one of the common causes of stump edema, it may occur because of bad bandaging, associated degenerative joint disease, poor venous return, kidney disease, and diabetes.
- How to control edema of the stump: Stimulation of limb in elevation with elastic bandage.
- Resisted exercise of the stump and other joints.
stump bandaging and conditioning:
- Bandaging plays an important role in conditioning and shaping the stump by reducing oedematous stump.
- 6 inches of elastic bandage was used for above-knee amputation. The elastic bandage should be taken off during exercise.
Principles of bandaging the stump:
- The pressure of the bandage should be mild firm and distributed evenly.
- Extra pressure is necessary at corners to maintain the conical shape of the stump. Pressure should be reduced proximally.
- During bandaging diagonal, oblique, or spiral turns should be used. In above-knee amputation, the bandage must extend up to the groin to prevent a roll of flesh from forming over the adductor tendons which may later lead to a follicle infection due to friction with the socket of the prosthesis.
- An above-knee stump should be bandaged with the position of the hip in extension and adduction.
Intermittent variable air pressure machine:
- Intermittent variable air pressure machine also called controlled air pressure machine.It is used to controle oedema by improving circulatuon of blood and lymph.
- Shrinker socks:oedema can be treated by elastic stump socks.
- Rigid dressing:Rigid plaster of paris dressing given to the patient with younge age.It also helps to reduced the oedema.
- stump hygiene: Stump hygiene includes regular washing of the stump with disinfected warm water soap and after dry the part.
- The amputed patient should be educated on protecting the areas and positions of affected limb.
- After Stitches removed: When the stitches are removed and the suture line healed satisfactory, the most important in amputation is stump conditioning.
stump conditioning :
- An ideal stump is perfect healed, firm, conical and with minimal flabby tissue.
- Bandaging: During elastic bandaging pressure and application should be proper.
- Exercise: Isometric exercise for the muscles of the stump, specially two joint muscles,which origenated above the joint proximal to the amputation
- Massage:massage can be helpful for improving tone of the muscles.
- Stimulation:Electrical stimulation with the stump elevation is used to decreased oedema and improve muscles tone.
- Pressure:Exposing the stump to pressure by either early use of pylon or gradual training weight bearing on the terminal weight bearing area of stump.It can be done by providing soft cushion and adjusting the height of the stool in the parallel bars.
Mobility Stage:
- Mobility stage is a stage of mobilization and restoration of functional independence.
- It start with crutch walking.Elderly patients may need initial ambulation practice in parallel bar.
- Mobilization and strengthening exercise :Mobilization of the body segment proximal Amputation.
- PNF techniques, Progressive resistance exercise and strong endurance exercise to the specific muscles groups are needed to facilitate effective body function with the prosthesis.
- Above knee amputation: Hip Flexion, abductors,Flexors and shoulder girdle muscles
Complications Of Amputation:
- Excess bleeding
- Blood clots
- Oedema
- Poor healing
- Deep vein thrombosis (DVT)
- wound infection
- pneumonia
- “phantom limb” pain
- depression
- Stump ulceration
- Flap necrosis
- Joint stiffness
- Osteomyelitis
- Osteoporosis
Prosthesis For Above Knee Amputation
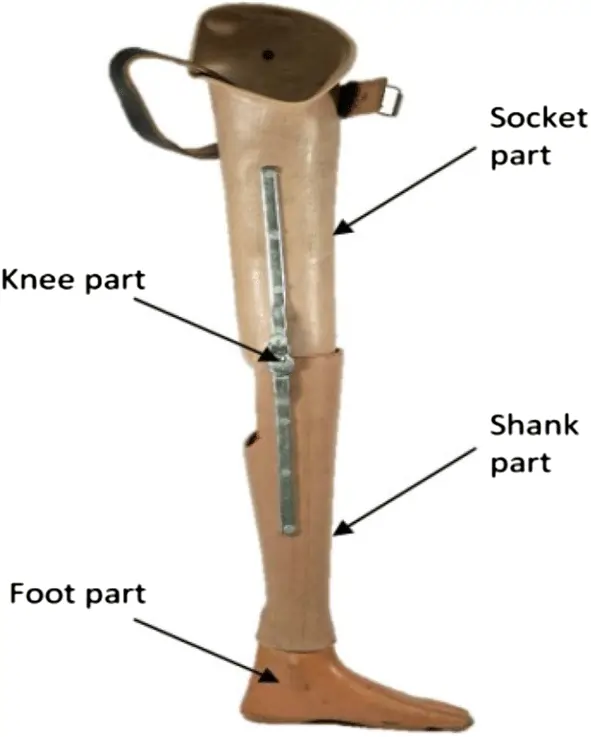
- The prosthetic design:
- Socket:
- Quadrilateral H-type socket, in which most of the weight of the body is transmitted through the ischial seat and then the posterior brim of the socket.
- Suspension:
- Suspension with a double swivel pelvic band with a multiaxial joint provides all movements at the hip joints. However, a rigid pelvic band only allows flexion, and extension is preferred in cases where muscle control and stability are deficient. Suction sockets with valve or modular prostheses are the alternative methods of the Above Knee prostheses.
- Knee Mechanism:
- Hand-operated or semi-automatic locking mechanism along with constant friction device or knee joint with a free mechanism in which swing can be given.
- Feet.Uniaxial or multiaxial SACH foot is preffered.It stimulates plantar flexion through the compression of a rubber heel. The uniaxial foot allows both dorsiflexion and planterflexion. The biaxial foot also allows eversion and inversion. The foot made of wood molded with plastic material is incorporated with rubber bumpers to provide necessary movements of joints.