
Limb-girdle muscular dystrophy (LGMD): Physiotherapy Exercise
Table of Contents
What is Limb-girdle muscular dystrophy?
Limb-girdle muscular dystrophy is a type of muscular dystrophy that affects the muscles of the shoulders, pelvis, lower arms, and legs. The first sign of the disorder is usually weakness or loss of function in the muscles that keep the shoulder in place (known as shoulder girdle muscles). Limb-girdle muscular dystrophy is one of the most common causes of weak muscles in young adults. Limb-girdle muscular dystrophy is inherited.
It is a term of a group of diseases that cause weakness and muscle wasting in the arms and legs. The proximal muscles which are close to the body are mostly affected mainly the muscles of the shoulders, upper arms, pelvic area, and thighs.
Types of LGMD
Type 1 LGMDs are dominantly inherited, require just one mutation for symptoms to result.
Type 2 LGMDs are recessively inherited, require mainly two mutations, one from a parent for symptoms to appear.
rarely, LGMDs are referred by their names, not by their numbers, and some types have not been assigned numbers.
The genetically found distinct subtypes have redefined the classification of LGMD and have led to nomenclature designating the autosomal dominant forms as LGMD1A, 1B, 1C, so on., and the autosomal recessive forms as LGMD2A, 2B, 2C, so on.
Causes of LGMD:
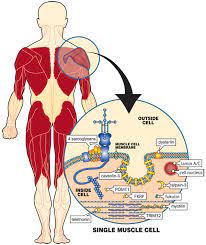
It is caused by genes mutations that result in abnormal function of proteins in muscles so that causing progressive muscular weakness.
The inheritance pattern of the condition varies and different genetic defects may result in the same clinical symptoms in different patients.
Sometimes, no obvious inheritance pattern can be recognized. Broadly, type 1 limb-girdle muscular dystrophy is dominantly inherited, and LGMD type 2 is recessively inherited.
Symptoms of LGMD :
Major symptoms of LGMDs are progressive weakness and muscle atrophy mainly in the shoulder girdle (scapulohumeral type), the pelvic girdle (pelvifemoral type), or both.
Distal muscle strength is usually preserved, even at the late stage of the disease, but distal muscle weakness can be an early or prominent feature in some LGMD subtypes.
Most childhood-onset cases have pelvicfemoral distribution of weakness.
The adult-onset disease generally includes both shoulder and pelvic girdles with gradually increased proximal limb weakness.
Weakness of facial muscles is usually mild or totally absent.
Strength of distal muscle is usually preserved, also in the end-stage of the disease, but distal muscle weakness can be an early or prominent feature in some LGMD subtypes.
generally, people who are suffering from LGMD first notice difficulty when they start to walk with a “waddling” gait due to the weakness of the hip and leg muscles.
muscles that control the movement of the eye around the eyeball, are totally spared in the LGMDs.
They may have difficulty in getting out of chairs, rising from a toilet seat, or climbing stairs.
Weakness in the shoulder area may have trouble to make reaching over the head, holding the arms outstretched, or carrying heavy objects. It may increase problems to keep the arms above the head for activities like combing hair or arranging things on a high shelf. Some people find it harder to type on a computer or keyboard and may even have trouble feeding by own.
limited mobility sometimes leads to muscle soreness and pain in the joints.
Respiratory (breathing) function can decrease over time, and it should be monitored regularly. There are some devices that may help improve respiratory function.
The involuntary muscles, except for the heart, which is a special type of involuntary muscle, are not affected in LGMD. Digestion, the function of bowel and bladder, and sexual function, which are carried out by involuntary muscles, remain normal.
Progression
Assistive devices, for instance, a cane or a long-hander, can make things easier as weakness progresses.
People whose LGMD has reached this level often recognized that a lot of their independence returns, and they have much less tired when they begin using this type of vehicle.
A power wheelchair or power cycle becomes convenient when weakness in the pelvic girdle and upper legs causes frequently falling.
Exercises to keep joints flexible, moving around as much as possible, warm baths, and, if needed, medication can keep this kind of discomfort to a minimum.
Diagnosis :
a doctor usually commences by taking a patient and family history and performing a physical examination.
The doctor also determines whether a patient’s weakness results from a problem in the muscles themselves as is the case in muscular dystrophy, or in the muscle-controlling nerves, called motor neurons, that control them.
A special blood test called a CK level. CK means creatine kinase, an enzyme that is leaking out of the damaged muscle. When elevated CK levels are found in a blood sample, it means the muscle is being destroyed by some abnormal process, such as muscular dystrophy or inflammation.
Special testing is called electromyography (EMG). In this test, the electrical activity of the muscles is measured, and nerves are stimulated to see where the problem lies.
A muscle biopsy, in that the surgical removal of a small sample of muscle from the patient. By examining muscle sample, doctors can tell a great deal about a potential diagnosis.
before doing muscle biopsy, less-invasive genetic testing is typically suggested.
Tests on the biopsy sample also can provide information regarding which muscle proteins are present in the muscle cells, and whether they are present in the normal amount and in the right locations.
DNA testing is available for several forms of LGMD and is expanding rapidly. If a particular type of LGMD is recognized, DNA testing from a blood sample may be undertaken relatively early in the diagnostic process, often before the doctor considers more invasive techniques.
Understanding inheritance patterns may be important for family planning. family history can help determine the inheritance pattern of the disorder.
Life expectancy
The progression of limb-girdle muscular dystrophy can vary among patients.For some, the disease progresses faster, leading to disability and affecting life expectancy.
For others, the progression of the disease is slow and might not affect life expectancy.
Recent research indicates that the age of onset of the disease may be predictive of how rapidly the disease will progress, with patients showing symptoms in childhood being the most severely affected.
Treatment of Limb-girdle muscular dystrophy :
Medical Management
The Rx of limb-girdle muscular dystrophy (LGMD) is supportive; no disease-modifying treatments are available.
Goals of Physiotherapy
To maintain mobility and functional independence
To manage associated complications, and maximize the quality of life, prevent contractures and maximize function for as long as possible.
Multidisciplinary management at centers with experience in neuromuscular disorders is recommended to provide optimal care.
Assistive devices:
Simple devices such as a cane or a long-handled reacher can make walking and accomplishing tasks easier as weakness progresses.
A power wheelchair or scooter becomes useful when weakness in the pelvic girdle and upper legs causes frequent falls. People whose LGMD has reached this stage often find that a great deal of their independence returns and fatigue is greatly reduced when they begin using this type of mobility equipment.
Heart, respiration, and diet
The heart can be affected in several LGMDs, including LGMD1B and LGMD2A-I, but this does not occur as often as it does in some other forms of muscular dystrophy.
Heart problems can take two forms — weakness of the heart muscle (cardiomyopathy) and abnormal transmission of signals that regulate the heartbeat (conduction abnormalities or arrhythmias).
The heart should be monitored for these complications with examination, electrocardiogram (ECG), and structural heart studies with echocardiography or cardiac magnetic resonance imaging (MRI) to guide management.
When necessary, medications or devices such as pacemakers can be used to treat heart complications. Heart transplantation may be needed for those who developed severe congestive heart failure.
Respiratory (breathing) function can decrease over time, and this also should be monitored regularly.
LGMD2I is associated with weakness of respiratory or oropharyngeal muscles and an increased risk of respiratory failure with disease progression.
Patients with LGMD who have evidence of respiratory insufficiency, daytime sleepiness, or symptoms of sleep-disordered breathing may benefit from noninvasive ventilation, which includes devices that can help sustain respiratory function.
Dysphagia means difficulty with swallowing and arm weakness associated with LGMDs can lead to malnutrition.
Patients with inadequate intake, swallowing problems, aspiration (when food, saliva, liquids, or vomit is breathed into the lungs instead of being swallowed into the esophagus), or weight loss should be evaluated with swallowing studies or referred to a gastroenterologist.
Such patients may benefit from different techniques to improve swallowing likewise, altering food consistency the use of a chin tuck maneuver, or the placement of a feeding tube.
No special dietary restrictions or additions are known to directly affect the span of LGMD. A doctor may advise a weight-reduction or weight-stabilization diet for some people because being markedly overweight puts greater stress on already-weakened muscles.
Physiotherapy exercise Video:
Physiotherapy rehabilitation exercises and occupational therapy programs are generally a significant part of the treatment for LGMD.
Occupational therapy mainly focuses on specific activities and functions, particularly the use of the hands, while physical therapy emphasizes mobility and where possible strengthening of large muscle groups.
Exercise protocol include simple exercises like sit to stand activity, sidestep, backward walk, marching in one place, step-ups, step-taps, step-overs, soccer kicks
Upper limb exercises – Straight sitting, scapular retraction, neck lateral flexion, neck retraction, shoulder rolls, shoulder resistive exercise, wrist movements, gentle gripping activities, range of motion exercises of the upper limb, reaching different targets,
Trunk exercises – Assistive crunches, trunk rotations, lateral bending of the trunk, picking up objects from the floor, log rolls
Lower limb exercises – Abduction of legs, quadruped walking, walking, donkey kicks, straight leg raise, knee walking, quadruped superman, low-intensity squats, sidewalks, toe taps on different points, crab walks, heel raises, toe raises
Co-ordination exercises – Shuffling cards, the opposition of thumbs, performing crafts, picking beads, writing
The primary goals of physical therapy are to allow greater motion in the joints and to prevent contractures. These problems can arise when movement is limited, so it is important for patients to continue to move as much as they can. These problems can arise when movement is limited, and it is important for the patient’s comfort and function to avoid them.
In occupational therapy, the focus is on improving abilities related to work, recreation, or daily living. For example, things like arm supports can make tasks such as using a computer or fixing your hair less tired.
In LGMD, certain kinds of stress-causing exercises may increase muscle damage. Patients with muscular dystrophy should maintain adequate hydration; avoid supramaximal, high-intensity exercise; and avoid exercising to exhaustion.
Some experts suggest swimming and water exercises as a good way to keep muscles as toned as possible without causing any undue stress. The water buoyancy helps protect against special kinds of muscle strain and injury. Before undertaking an exercise program, make sure you have had a cardiac evaluation, and do not swim alone. For more on exercise, see Exercising with a Muscle Disease.



This is helpful to watch the exercise and workout, but it would help greatly to have speaking in English. U.S. English.
Thank you for posting.