
Pectoralis Major Muscle
Table of Contents
Pectoralis Major Muscle Anatomy
The pectoralis major is a prominent muscle located in the chest region of the human body. It is a large, fan-shaped muscle that plays a crucial role in the movement of the shoulder and arm.
If you enjoy working out, you may also hear people refer to these muscles as the pecs. The clavicular part, sternocostal section, and abdominal part are the three divisions of the pectoralis major, which has a broad origin.
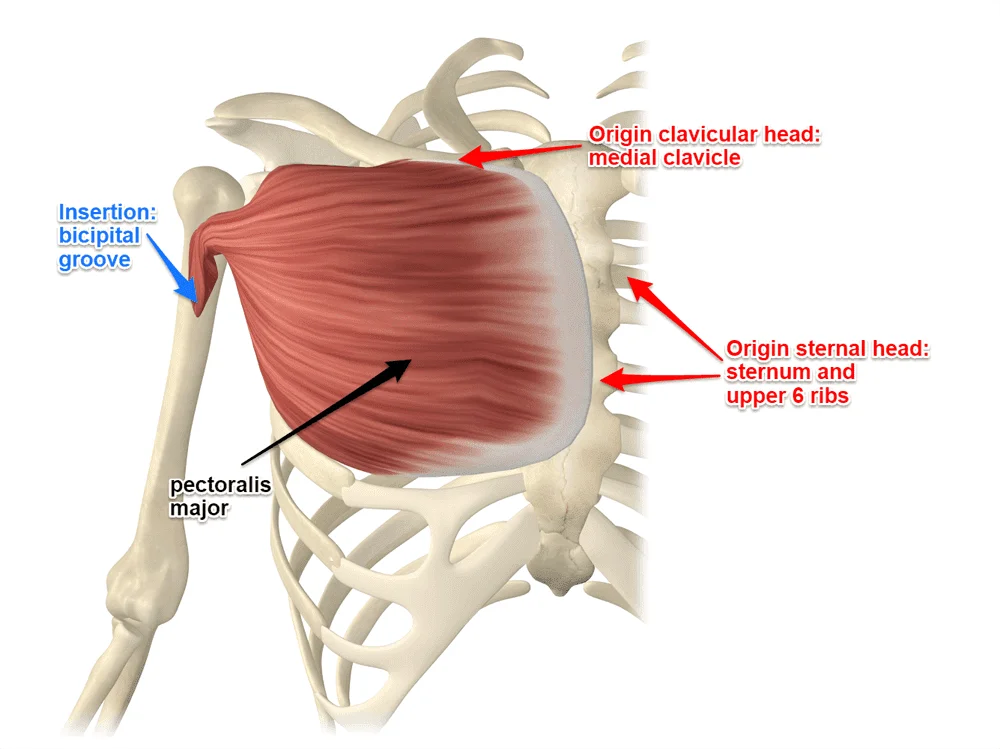
The aponeurosis of the external oblique of the anterior abdominal wall, the anterior side of the sternum, the sternal end of the sixth rib, the anterior surface of the medial half of the clavicle, and the first seven costal cartilages are where it originates.
The lateral lip of the humerus’s intertubercular sulcus is where the pectoralis major inserts. The clavicular and sternocostal heads of the pectoralis major are named after their respective regions of origin. It is said that the sternocostal head is divided into two to seven separate segments.
Origin
Clavicular part: Front surface of the medial half of the clavicle
Sternocostal part: the sternum’s anterior surface, ribs’ costal cartilages 1–6
Abdominal part: Anterior layer of the rectus sheath
Insertion
it is inserted by a bi-laminar tendon on the lateral lip of the bicipital groove
the two laminae are continuous with each other inferiorly.
Nerve supply
medial and lateral pectoral nerves.
There are distinct neural supplies to the two heads of the pectoralis major. The lateral pectoral nerve provides the clavicular head with its nerve supply. The sternocostal head supply by the medial pectoral nerve. The brachial plexus’s lateral cord gives birth to the lateral pectoral nerve, whereas the medial cord gives birth to the medial pectoral nerve.
The medial chord will go to the pectoralis minor, and the lateral cord will go anteriorly to the axillary artery. After that, it passes through the pectoralis major’s posterior side and enters the muscle medial to the humeral insertion. The pectoralis minor is punctured by the medial pectoral nerve, which originates posterior to the axillary artery and enters into the pectoralis major posterior surface in many branches.
Blood supply
Therefore, the lateral artery, the pectoral branch of the thoraco-acromial artery, and, to a lesser extent, the superior thoracic artery deliver blood to the pectoralis major muscle.
Lymphatic Drainage
The subclavian vein receives its venous drainage from the pectoral vein.
Action
Acting as a whole the muscle causes abduction and medial rotation of the shoulder.
clavicular part produces flexion of the arm.
sternocostal part is used in:
– an extension of the flexed arm against resistance.
– climbing.
Function
The pectoralis major has three functions, depending on the muscle heads that are engaged.
The pectoralis major serves as a powerful adductor and internal rotator of the humerus at the shoulder joint when the arm is in the anatomical position. The clavicular part of the muscle flexes the humerus up to ninety degrees in a horizontal plane on its own. The antagonistic movement that returns the humerus to its anatomical place might be produced by the sternocostal part of the muscle.
Relations
The anterior chest wall contains the broad superficial muscle known as the pectoralis major. In men, the surrounding skin, subcutaneous tissue, and a thick layer of fascia protect it. It is hidden by the breast in females. The anterior surface of the upper six ribs, as well as the pectoralis minor and serratus anterior muscles, are covered by the deep surface of the muscle.
The infraclavicular fossa, also known as Mohrenheim’s fossa, is a triangular depression that lies between the clavicle, deltoid muscle, and pectoralis major muscle. It is a crucial landmark for subclavian artery surgery.
Embryology
The mesoderm, one of the three germ layers, is where the skeletal muscles develop. The paraxial mesoderm is arranged in tissue blocks known as somites alongside the neural tube throughout the fourth and eighth weeks of development.
The dorsolateral dermomyotome and the ventromedial sclerotome are the two cell subpopulations found in the somites. The skeletal muscle is then formed by the dermomyotome. At this stage, the axial skeleton is formed by the sclerotome. The hypomere cells in the dermatomyotome give rise to the anterior muscles of the developing embryo.
Poland syndrome is characterized by pectoral muscular congenital anomalies. This is typified by the unilateral lack of the pectoralis major, which typically coexists with other chest wall abnormalities and ipsilateral symbrachydactyly.
Exercise of Pectoralis Major Muscle
Strengthening exercise:
The pectoralis muscle is the target of many exercises. Among the most popular are pressing exercises: The pectoralis major muscle is used in both the flat dumbbell bench press and the flat barbell bench press. The person performs both exercises while lying supine on a bench with their feet flat on the floor. The person extends their arms and slowly lowers a barbell or a pair of dumbbells towards their nipple line. They then raise the weights to about arm’s length above their face.
For the dumbbell fly exercise, which can also be performed on an incline bench, the person must lie supine with their feet flat on the floor on a bench. With your arms slightly bent and internally rotated so that your elbows face outward, raise dumbbells above your chest. Dumbbells should be lowered to the sides while keeping your arms slightly bent. Return the dumbbells to their initial position above the chest to complete the workout.
- Pushups. Pushups are the most obvious choice because they require no special equipment and can be done anywhere.
- Dumbbell press. Somewhat like a bench press, the dumbbell press is another good choice for building pectoral muscles.
- Bench press.
Stretching exercise of Pectoralis Major Muscle

Stand in the middle of a doorway with one foot in front of the other. Bend your elbows to a 90-degree angle and place your forearms on each side of the doorway. Shift your weight onto your front leg, leaning forward, until you feel a stretch in your chest muscles. Hold for 10-15 seconds then switch sides.
Surgical Importance
Owing to its size, position, and blood supply, the pectoralis major has been utilized in neck surgery flap repairs. Because of the thoracoacromial artery’s high vascularization, the muscle has a decreased risk of necrosis during the development of the flap.
The emergence of vascularized free flaps has led to a decrease in the use of pectoralis major myocutaneous flaps (PMMC). Nonetheless, it is a dependable choice for soft tissue repair of the face and neck after surgeries due to tumors or injuries. The oropharyngeal, pharyngoesophageal, skull base and head and neck deformities can all be closed using the PMMC. It can also be used to cover exposed vascular. Additionally, the flap may give severe neck dissection more mass.
A thorough understanding of the pectoral muscle’s anatomy is especially important for breast surgery. The pectoralis major nerve supply may be endangered by a modified radical mastectomy, breast reconstruction after mastectomy, and breast augmentation.
A portion of the pectoralis major may atrophy or fibrosis as well as denervation if the nerve is damaged. Another more popular form of analgesia following surgery is pectoral nerve blocks. It is thought to be less intrusive and to cause fewer problems than neuraxial or paravertebral blocks.
Clinical Importance
Pectoralis injury
Pectoralis injuries are rather uncommon; a 2012 meta-analysis found that 365 occurrences had been documented in the literature. About half of the tendon tears that occur in men between the ages of 20 and 40 are caused by weight-bearing activities like the bench press, which needs the arm to be in extension and external rotation. Swelling, hemorrhage, medialization of the muscle bed, and soreness at the humeral insertion and axilla are all signs of a pectoralis major rupture.
These symptoms are nonspecific and can appear suddenly or gradually over several weeks. Radiography and clinical history and examination are the main areas of focus for the investigation of possible pectoral injuries. Bony injury (avulsion occurring in 2% to 5% of instances) can be ruled out with a chest x-ray, and tears can be diagnosed and characterized with great accuracy using ultrasound and magnetic resonance imaging.
Tietjen proposed a categorization system for pectoralis major injuries in 1980.
Grades are I to III,
- Grade I: A contusion or sprain
- Grade II: A small tear
- Grade III: Total tear of the musculotendinous junction, the muscular belly, the sternoclavicular origin, and the insertion
The majority of tears are conservatively treated with cold packs, analgesics, and immobilization in an internally rotated sling. From two to six weeks, the patient may progressively improve their level of movement. After 6 to 8 weeks, mild resistance exercises can be added, and after 3 to 5 months, a complete return to resistance exercises is feasible.
However, surgical repair is suggested and should ideally be carried out within six weeks of the injury in situations of full tears or in the young and athletic population. The best method to regain maximum strength, mobility, and function for young people and athletes is through surgical repair.
Poland syndrome is an embryonic malformation of the thoracic wall, which is accompanied by a defect of the pectoralis major muscle in combination with other malformations of the upper extremities (e.g. malformations of the fingers). The muscle can be partly or completely missing. Depending on the degree of severity, the adduction and internal rotation of the shoulder joint are more or less difficult to perform (for example, the crossing of the raised arms).
In addition, affected patients have visibly distorted breasts due to the aplasia of the pectoralis major muscle, which is why a plastic-surgical reconstruction can be used therapeutically.
Chondro epitrochlearis:
Chondroepitrochlearis (CET) is an anomalous muscular slip that originates from the pectoralis major muscle and inserts into the epicondyle of the humerus. The morphology of this variant form of pectoralis major can vary from slender to strong musculo-tendinous. In its course, it usually crosses the neurovascular structures of the arm; their compression is a major complication that could be manifested by its persistence. In the present case, a potentially anomalous CET muscle with a slender slip of origin, but strong tendinous insertion to the medial epicondyle of the humerus was found unilaterally.
This musculo-tendinous structure was found to be compressing the brachial artery and median nerve in the arm. A detailed embryological and clinical perspective of such variant muscular slip helps physiotherapists, and orthopedics in their treatment strategy for complaining of restricted shoulder movement. It may also help the neurologists, and radiologists in their diagnostic approach of ulnar neuropathy.
Trigger Points
The symptoms of angina pectoris or a heart attack might be quite similar to those caused by trigger points in the pectoralis major muscle. These trigger points can cause pain that is referred to the inside of the elbow, down the inside of the arm, in the front of the shoulder, and in the chest. They could also result in hypersensitivity in the nipples and breast soreness.
FAQ
The largest and most superior muscle of the anterior chest wall is the pectoralis major. It is a thick, fan-shaped muscle that forms the anterior wall of the axilla and is located beneath the breast tissue.
4 pectoral muscles are:
Pectoralis major.
Pectoralis minor.
Serratus anterior.
Subclavius.
The pectoralis major contracts to pull on the humerus to produce lateral, vertical, or rotational motion, which is mostly utilized to control arm movement. In order to make room for the lungs to expand during deep inhalation, the pectorals pull the rib cage.
It is in charge of the adduction, flexion, and medial rotation of the humerus, which are the movements of the shoulder joint. It contributes to the stabilization of the shoulder joint as well. Beneath the pectoralis major is the larger muscle known as the pectoralis minor.
The largest muscle in the pectoral region, the pectoralis major, is a thick, fan-shaped muscle located above all other muscles in the chest beneath the breast. The Latin words pectoralis, which means of the breast, and pectus, which means breast, are the sources of the English word pectus.
The location and size of the pectoralis major muscle are the two factors that give it its name. The term “major” designates the greatest muscle, whereas “pectoral” refers to the chest. Consequently, the literal translation of the pectoralis major “major muscle is the largest muscle of the chest”.
15 Comments