
Abductor Pollicis Longus Muscle
Table of Contents
Abductor Pollicis Longus (APL) Muscle Anatomy
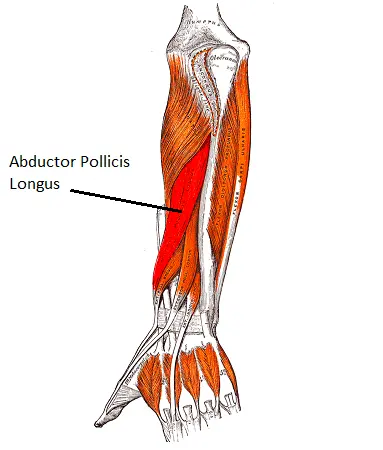
The Abductor pollicis longus muscle lies immediately below the supinator and is sometimes united with it. It is found in the posterior compartment of the forearm. It is one of the five deep extensors in the forearm, along with the supinator, extensor pollicis brevis, extensor pollicis longus, and extensor indicis.
Origin
It originates from the posterior surface of the proximal half of the radius, ulna, and interosseous membrane.
A thin tendon emerges from the muscle just proximal to the wrist. This tendon joins the tendon of the extensor pollicis brevis muscle in a groove carved on the lateral side of the distal end of the radius.
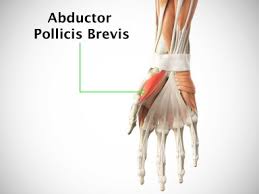
The extensor retinaculum is therefore just beneath the abductor pollicis longus tendon. It passes through the retinacular space’s initial dorsal (extensor) compartment in the process. The tendon separates into two slips as it reaches the hand’s dorsum, inserting onto the base of the trapezium and first metacarpal bones, respectively. A few fibres may also enter into the fascia of the thenar eminence, the opponens pollicis, and the abductor pollicis brevis.
Insertion
It inserts on the base of the first metacarpal bone.
Nerve supply
The posterior interosseous nerve supplies the muscle.
Blood supply
The Posterior interosseous artery and anterior interosseous artery supply the muscle.
Action
It acts as an extensor of the hand at the radio-carpal joint and as a thumb extensor and abductor at the carpometacarpal joint.
The muscle aids in the complete extension of the thumb at the metacarpophalangeal joint, working in coordination with the thumb’s long and short extensors. This movement is crucial when releasing your grip on anything, such as an object you are holding. At the radiocarpal joint, the abductor pollicis longus aids in the radial deviation, or abduction, of the hand.
Relations
The distal portion of the posterior forearm includes the abductor pollicis longus muscle bellies. Its tendon is situated lateral to the tendon of the extensor pollicis brevis, and it is situated deep to the extensor digitorum and lateral to the extensor pollicis longus muscle. Between the abductor pollicis longus and extensor digitorum, the posterior interosseous nerve and artery cross the superficial surface of the abductor pollicis longus.
The anatomical snuffbox’s lateral border is formed by the tendon of the abductor pollicis longus. This triangle-shaped area is situated distal and posterior to the radius’s styloid process near the base of the thumb. The hand’s neurovascular structures—the cephalic vein, radial artery, and superficial branch of the radial nerve—pass via the anatomical snuffbox. The scaphoid and trapezium bones make up the floor, while the extensor pollicis longus (lateral) and brevis (medial) complete the edges of this area.
Variations
More than 80% of individuals have an additional abductor pollicis longus (AAPL) tendon, and 20% have a distinct muscular belly. In one research, the accessory tendon was put into the trapezium (41%); proximally on the base of the first metacarpal (1%); additionally inserted on the trapezium and thenar muscles (15%); and proximally on the abductor pollicis brevis (22%) and opponens pollicis brevis (5%). Rare occurrences have been documented involving up to seven tendons.
Since healthy tendons may compensate for damaged ones, having many APL tendons might be considered a functional benefit.
Clinical Relevance
The most important clinical condition involving the Abductor Pollicis Longus(APL) muscle, usually along with the Extensor pollicis brevis (EPB) is DeQuervain’s Syndrome. It is characterized by thickening and inflammation of tendons of APL and EPB resulting in pain and swelling in the first extensor compartment of the wrist.
Strengthening exercise
Stretching
The abductor pollicis longus is stretched with adduction and flexion of the thumb at the carpometacarpal joint and radial deviation of the hand at the wrist joint.
Assessment
The individual is asked to abduct the thumb while maintaining a neutral forearm posture in order to evaluate the strength of APL. In the direction of the thumb’s adduction, resistance is exerted on the lateral side of the distal end of the first metacarpal.
Finklestein’s test is the one used to diagnose DeQuervains clinically. Thumb within fingers, the patient is urged to create a fist. The wrist is passively shifted to the ulnar side by the therapist/examiner. Pain above the radial styloid process, where the tendons of the APL and EPB are located, indicates a positive test.
FAQs
The primary function of the abductor pollicis longus is to move the thumb anteriorly by abducting it at the carpometacarpal joint. It also helps with thumb rotation and extension. It assists in flexing the hand and abducting the wrist (radial deviation) as it continues to work.
The posterior interosseous nerve (C7, C8), a continuation of the radial nerve’s deep branch, innervates the abductor pollicis longus.
omes from the neighbouring posterior surfaces of the ulna and radius as well as the interosseous membrane. It attaches to the first metacarpal’s lateral side at the base. Thumb abduction is the action.
7 Comments