
Extensor Pollicis Longus Muscle
Table of Contents
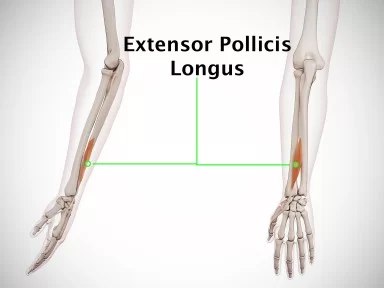
Extensor Pollicis Longus Muscle Anatomy

The extensor pollicis longus (EPL) is a thin muscle of the forearm that belongs to the posterior muscle group, lying in the second or deep layer.
The extensor pollicis longus (EPL) muscle is an extrinsic thumb muscle that adducts and extends the thumb’s metacarpophalangeal (MCP) and interphalangeal (IP) joints. It plays a significant role in thumb function. The EPL is supplied with blood by the radial, ulnar, anterior, and posterior interosseous arteries. It is a nerve supplied by the posterior interosseous nerve.
Origin:
It originates from the posterior surface of the middle third of the ulna and interosseous membrane.
Insertion:
It inserts on the posterior aspect of the base of the distal phalanx of the thumb.
Nerve supply:
The posterior interosseous nerve innervates the muscle.
Blood Supply:
The Posterior interosseous artery supplies the muscle.
Action:
It acts as a weak extensor of the hand and a strong extensor of the thumb.
Function:
The main action of extensor pollicis longus is the extension of the thumb at the metacarpophalangeal and interphalangeal joints. Extension at the metacarpophalangeal joint occurs in synergy with the extensor pollicis brevis muscle. When the thumb reaches the full extension or abduction, the extensor pollicis longus can also assist in the adduction of the thumb.
Strengthening Exercise:

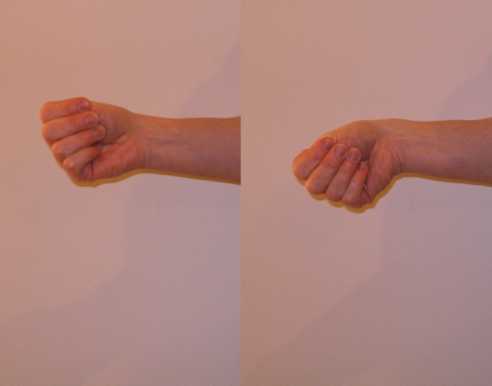
- Wrap the rubber band around all your fingers, having it rest right above your knuckles. Have your elbow resting on a surface like the arm of a chair or a table.
- When you’re ready, open your hand against the resistance of the rubber band and then slowly turn back into the closed finger position.
- Hold your movement at the open position for a moment before retracting back. Repeat for 3 sets of 10 reps. Make sure to switch hands.
Stretching Exercises:
- Hold onto your thumb firmly with your other four fingers.
- While keeping your wrist in a neutral position, turn your wrist down toward the floor.
- A mild stretch will feel near the thumb.
- Hold this position for 30 seconds
- then release it.
- Repeat the exercise 3 times.
Anatomical Variations
Using Turker Classification, variations of the extensor pollicis longus can be classified.
- The patient has an additional muscle that attaches separately from the EPL at the base of the distal phalanx of the first digit. Its tendon passes through the fourth dorsal compartment and joins the extensor pollicis longus tendon at the first metacarpal mid-shaft.
- Patients have an additional muscle that attaches separately from the EPL at the base of the distal phalanx of the first digit, with its tendon running alongside the extensor pollicis longus in the third dorsal compartment.
- There is an additional muscle in the patient, and its tendon passes into the fourth dorsal compartment before inclined and running parallel to the extensor pollicis longus until joining the distal EPL tendon.
- Patients have an additional muscle whose tendon passes through the fourth dorsal compartment, crosses the extensor carpi radialis tendons, goes over the EPL, and attaches to the first digit’s proximal phalanx in an oblique way.
- The extensor pollicis and indicis communis, which originates on the ulna between the extensor pollicis longus and extensor indicis, is an additional muscle present in patients. One slip runs alongside the thumb’s EPL, while the other slip runs alongside the index finger’s extensor indicis. This muscle splits these two slips. On the distal phalanx, the slip that runs parallel to the EPL on the thumb inserts at the same spot.
- The patient has a single belly from the extensor pollicis longus muscle, which results in the radial and ulnar slips of the EPL tendon. The ulnar and radial slips cross the extensor retinaculum and first and second extensor compartments, respectively. The metacarpophalangeal joint reunites them, and they proceed in the direction of the distal phalanx.
- Patients have a belly of the extensor pollicis longus muscle, which results in two distinct EPL tendon slips that run inside the third extensor compartment.
Embryology
The forearm musculature arises from the differentiation of the precursor extensor muscle mass into three distinct sections. The extensor carpi radialis longus, brevis, and brachioradialis originate from the radial part. The extensor digitorum communis, extensor carpi ulnaris, and extensor digiti minimi originate from the superficial part. The abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis originate from the deep part.
While there are notable variances in the deep part of the extensor muscle mass between different monkey species, the radial and superficial portions of this muscle mass appear to be well conserved, which may account for the wide range of variability found in the muscles and tendons in that region. With a prevalence of only 1%, mutations of the EPL are, nevertheless, quite uncommon.
Clinical Importance
Drummers palsy
Inflammation or a rupture of the extensor pollicis longus tendon is commonly referred to as “drummer’s paralysis”. This condition is most commonly caused by blunt mechanical injuries to the wrist area or a simple overuse of the extensor pollicis longus muscle. It is most commonly seen in drummers, sculptors, blacksmiths, or waiters. This condition results in weakness of the extensor pollicis longus, which is presented as an incomplete extension of the thumb.
Tenosynovitis, or inflammation of the synovial tendon sheath enveloping tendons, is frequently seen in the tendons of the abductor pollicis longus and extensor pollicis brevis, which are located in the wrist’s first extensor compartment. It is uncommon to see it in the other extensor compartments in people without rheumatoid arthritis. On the other hand, tenosynovitis of the EPL synovial tendon sheath in the third extensor compartment has been documented in some cases.
Following repetitive wrist or thumb motions, patients frequently suffer from vague wrist pain. Tenderness along Lister’s tubercle and the EPL tendon may also be evident. Patients may experience discomfort when their first digit IP joint is in passive motion. This is a difficult diagnosis to make because it may take months for the pain to become localized to the third extensor compartment. The fact that every patient in the few case reports on this illness had an EPL musculotendinous junction that stopped inside the third extensor compartment suggests that the tighter compartment may have increased the patient’s susceptibility to tenosynovitis.
One-sixth of all fractures treated in the ER are distal radius fractures. A rare yet well-recorded consequence of adult non-displaced distal radius fractures is an EPL rupture that occurs a few weeks after the fracture. The third extensor compartment is compressed, resulting in ischemia, irritation, and EPL degeneration, all of which are hypothesized processes for the ruptured EPL. Hemostasis and callus formation following the fracture are other contributing factors.
It’s crucial to assess the integrity of a patient’s EPL when they have a distal radius fracture diagnosis and return a few weeks later complaining of being unable to actively initiate thumb extension at the MCP and IP joints despite having a full passive range of motion. Generally speaking, it’s critical to consider EPL tendon rupture in the differential diagnosis when patients exhibit a complete passive range of motion with extension but limited active thumb extension at the MCP and IP joints. Patients experiencing a rupture may experience a popping sensation and discomfort over the tubercle in Lister’s disease.
It is crucial to rule out any general medical disorders that may be connected to thumb muscle hypoplasia in patients who may appear with the EPL tendon placed on the radial side of the proximal phalanx. Examples include Cornelia de Lange syndrome, which also manifests as dwarfism; Okihiro syndrome, which also manifests as impaired eye movement and deafness; Fanconi anemia, which also manifests as pancytopenic anemia; and Holt-Oram syndrome, which also manifests as congenital heart defects.
If the avulsed fragment is not correctly fixed, patients who suffer avulsion fractures of both metacarpals at the insertion of the extensor carpi radialis longus tendon may experience a rupture of their EPL tendon. In order to avoid complications, individuals with avulsion fractures at the insertion of the extensor carpi radialis longus tendon must have their fracture fragments internally fixed.
Surgical Importance
EPL tenosynovitis
There hasn’t been a single case of extensor pollicis longus stenosing tenosynovitis that has been successfully treated non-operatively, thus individuals with this rare condition probably need surgery. Furthermore, concerns about EPL tendon rupture with chronic deterioration are inextricably tied to the significance of surgical treatment for EPL tenosynovitis, as previously argued in the literature. The EPL tendon must be fully released and translated into the subcutaneous tissue on the radial aspect of Lister’s tubercle in order to accomplish the surgical repair. Tenosynovitis recurrence, tendon bowstringing, and function compromise are avoided by transposing the EPL tendon.
Dorsal or volar plating methods may be used as a surgical treatment for displaced distal radius fractures that require open reduction and internal fixation (ORIF). Patients undergoing treatment with a dorsal plate are more likely to experience iatrogenic damage, or mechanical irritation of the tendons, resulting in a rupture of the extensor pollicis longus tendon in the wrist and hand. While iatrogenic extensor tendon injury has been made less likely by technological developments in low-profile dorsal plating procedures, this complication is still a known concern.
Tendon transfers
Patients may receive a free tendon graft or a tendon transfer if they need surgical reconstruction for a ruptured extensor pollicis longus tendon. In addition to the palmaris longus, extensor carpi radialis longus, extensor carpi radialis brevis, and abductor pollicis longus, other tendons that are useful for tendon transfer are the extensor indicis. Even though the palmaris longus tendon is avascular, it can be transferred to maintain index finger extension power, which often declines following an extensor indicis tendon transfer. Ensuring the repaired tendon is properly tensioned is crucial since an excessive amount of tension will cause the thumb to become hyperextended and unable to flex.
There will be deficits in extension if there is insufficient tension. Placing the patient’s hand on the table with their forearm pronated and their wrist in a neutral posture allows the surgeon to roughly determine the ideal tension. The patient’s thumbnail edge’s center of mass should be measured. There should be a 2 cm gap. In order to achieve the proper tension in the repaired EPL and keep the thumbnail edge 2 cm off the table, the reconstruction should be removed and redone if the suturing is essentially keeping everything together.
The stability of the extensor pollicis longus tendon depends on the thumb’s sagittal band, particularly its radial component. The radial and ulnar components of the sagittal band, as well as the nearby tendinous structures like the extensor pollicis brevis and EPL, may sustain injury from lacerations that occur close to the thumb’s MCP joint. Consequently, as the radial sagittal band serves to anchor the EPL tendon, it is imperative that the injured components be repaired, particularly if there has been damage to it.
The EPL tendon may subluxate if the radial sagittal band is not surgically corrected. Rheumatoid arthritis patients may experience both radial sagittal band weakening and contracture of the ulnar sagittal band. In the end, that can result in a thumb boutonniere malformation. The boutonniere deformity may be treated in patients with early rheumatoid arthritis by surgically releasing the contracting ulnar sagittal band and strengthening the radial sagittal band by supplementing it.
Most EPL tendon abnormalities do not cause wrist or hand pain or impairments in thumb extension in their patients. Anomalies of the EPL tendon are frequently discovered following surgery to treat another wrist or hand condition. In those situations, since the patient is asymptomatic, surgical surgery is not recommended. To lessen the degree of EPL tendon compression within the extensor compartment, surgical treatment using techniques like an extensor retinaculum release and Lister’s tubercle excision is recommended when patients are experiencing discomfort.

6 Comments