Palmar Interossei Muscle
Table of Contents
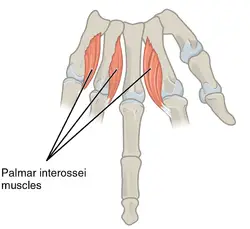
Palmar interossei Muscle Anatomy
The palmar interossei muscle or volar interossei (interossei volares in older literature) are three small, unipennate muscles in the hand that lie between the metacarpal bones and are attached to the index, ring, and little fingers. They are smaller than the dorsal interossei of the hand.
Origin
The palmar interossei origins are
- 1st interossei arises from the medial side of 1st metacarpal.
- 2nd interossei arises from the medial side of 2nd metacarpal.
- 3rd interossei arises from the lateral side of the 4th metacarpal.
- 4th interossei arises from the lateral side of the 5th metacarpal.
Insertion
It inserts on the bases of proximal phalanges and on its extensor expansions.
Nerve supply
The deep branch of the ulnar nerve supplies the muscle.
The ulnar nerve’s deep branch supplies the palmar interossei with nerve fibers. T1 is the principal innervating segment, and nerve roots of C8 and T1 give rise to the deep branch of the ulnar nerve.
Lymphatic Drainage
There are two types of lymphatic drainage in the upper limbs: superficial and deep lymphatic drainage. The skin’s lymphatic plexuses on the palm and dorsum of the hand ascend to the axillary and cubital lymph nodes in tandem with the basilic and cephalic veins, respectively. The humeral lymph nodes are the final destination of deep lymphatic vessels, which originate from the principal deep veins.
Blood supply
It receives arterial blood supply from the branches of the deep palmar arch.
Action
The main function of palmar interossei is to adduct the fingers in a longitudinal axis, which means the movement of the fingers towards the middle finger.
Function
The main function of palmar interossei is to adduct the fingers in a longitudinal axis, which means the movement of the fingers towards the middle finger.
Specifically, the 1st palmar interosseous pulls the index finger medially, whereas the 2nd and 3rd pull the ring and little fingers laterally.
Functionally, the palmar interossei are antagonists to the dorsal interossei in the metacarpophalangeal joint.
In addition, palmar interossei greatly contribute to flexion at the metacarpophalangeal joint, and extension at the interphalangeal joints of the 2nd, 4th, and 5th finger.
Structure
The metacarpals of the corresponding digit are the source of the unipennate muscles known as the palmar interossei. Through the third digit, these muscles adduct the first, second, fourth, and fifth digits about a long axis. The metacarpophalangeal joints are the site of the adduction. Furthermore, the flexion at the metacarpophalangeal joints and the extension at the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the corresponding fingers are facilitated by the palmar interossei.
The first palmar interossei, when present singly, inserts into the base of the proximal first phalanx, the extensor hood, and the first phalanx. It begins at the medial, palmar surface of the first metacarpal. Most anatomy textbooks classify the first palmar interosseus as rudimentary, believing it to be a part of the flexor pollicis brevis or the adductor pollicis. This idea, however, has been refuted by recent research, which discovered that over 85% of specimens contain the first palmar interossei, also known as the “pollical palmar interosseous.” These findings imply that this muscle, which is believed to have originated from the adductor pollicis’ oblique head, was involved in the evolution of humans.
The base of the first phalanx and the medial section of the first digit’s extensor hood are where the second palmar interosseous inserts after starting at the medial surface of the second metacarpal.
The lateral aspect of the fourth and fifth metacarpals is where the third and fourth palmar interossei begin, and they insert into the lateral aspect of the corresponding extensor hood. They also insert into the base of the proximal phalanx in each case.
Relations
The palmar interossei muscles are located between the metacarpal bones on the palmar surface of the hand. They are smaller than the dorsal interossei muscles.
The oblique head of the adductor pollicis anteriorly and the first dorsal interosseous posteriorly are the locations of the first palmar interosseous.
The oblique head of the adductor pollicis overlaps the second palmar interosseous as well, while the flexor digitorum profundus tendons meant for the ring and little finger covers the third and fourth palmar interossei.
Assessment
Studies on nerve conduction velocity and electromyography are performed to assess ulnar nerve disease and rule out other diagnoses.
Patients with a positive Wartenberg’s sign are told to adduct all of their fingers. In the event of a positive test, the fifth finger will abduct in relation to the other digits, suggesting weakening in the fourth lumbrical and third palmar interosseous muscles.
Method: To assess palmar interossei weakness, a patient can be taught to hold a piece of paper between any two or all five fingers. If the paper falls out, this indicates a weakness in the palmar interossei.
Strengthening exercise:
Isometric Finger Adduction Exercise

- Sit upright in a chair.
- Place your affected arm on a table with your palm facing down and your fingers flat.
- Place a finger from your unaffected hand on the side of your finger that is closest to your middle finger.
- Try to move your affected finger in towards your middle finger, using your opposite hand to resist the movement.
- Remember to keep your palm and forearm flat on the table throughout the exercise.
- Repeat the same with the other fingers.
Stretching exercise:
Embryology
Four limb buds emerge from the somites and mesenchyme of the lateral plate mesoderm at the conclusion of the fourth week of embryonic development. This mesenchyme is then coated in an ectoderm layer. Numerous protein factors contribute to the development of the upper limbs, but two in particular—fibroblast growth factors (FGF) and sonic hedgehog (Shh)—are essential. Anteroposterior, dorsoventral, and proximo-distal are the three spatial limb axes that are developed as a result of the interactions between these different proteins and their respective gene expressions.
Around days 34–38 of embryonic development, the distal upper extremity buds flatten to start the development of the hand. While the mesenchyme of the lateral plate mesoderm generates bone and cartilage, somites form the muscle of the limbs. The hand’s somitic mesoderm is divided into layers that are superficial and deep. This mesoderm’s deep layer gives rise to the palmar and dorsal interossei muscles. Tendons reach full development and functionality by the twelfth week of development.
Anatomical Variantions
In most anatomy classes, students are taught that all palmar interossei have one head, which is referred to as a unipennate head. It was discovered in a retrospective research that only about 62% of palmar interossei were unipennate.
The results of this study also indicate that the attachment sites of the palmar and dorsal interossei, which have a great deal of diversity, have been oversimplified in textbooks. Distal insertions into any part of the volar plate, bony attachment, extensor hood, or a combination of these locations are included in this variety.
As was previously indicated, the majority of modern anatomy textbooks instruct that the first palmar interosseous muscle is rarely functioning on its own and is typically a part of the flexor pollicis brevis or adductor pollicis. Henle (1858) was the first to propose that the first palmar interosseous muscle is an independent, intrinsic hand muscle, and other recent research have confirmed this idea. After dissecting 72 hands, one study discovered that 67 hands (93%), contained the first palmar interosseous, also known as the “pollical palmar interosseous” (PPI) muscle of Henle.
After examining six additional comparable trials, the authors discovered that the PPI was present in more than 80% of cadaveric hands. Due to its major contribution to the thumb’s dexterity, researchers believe that the presence of the PPI in humans had a substantial impact on the evolution of the human species from non-humanoid primates.
Surgical Considerations
Hand surgery is the standard therapy for metacarpal fractures, with a metacarpal shortening range of 2mm to 10mm. Researchers have discovered that the corresponding interossei’s strength decreases by about 8% with a 2 mm metacarpal shortening. Furthermore, the corresponding interossei strength can be decreased by approximately 55% with a 10mm shortening.
Interossei compartment syndromes are comparatively uncommon and usually result from acute ischemia, crush injuries, or burns. A case study detailed the experiences of two kids who had suction injuries after getting their hands entangled in a swimming pool’s intake pipe filter. Acute interossei compartment syndrome was brought on by this system, necessitating immediate surgical decompression. The authors made two incisions, one between the middle and ring fingers and the other between the index and middle fingers, as mentioned in other articles that detail the process.
The dorsal interossei were freed by dissection along the sides of the metacarpals, and the adductor compartment and the first palmar interossei were released by further dissection down the index metacarpal. The remaining palmar interossei were freed by thorough dissection along the radial and ulnar sides of the ring metacarpal.
Clinical relevance:
The palmar interossei receive innervation from the deep palmar branch of the ulnar nerve. so,
1.) Injury to the ulnar nerve can manifest as weakness or even atrophy of the interossei muscles and is mainly caused by:
nerve root impingement
brachial plexus compression
nerve entrapment at the elbow, forearm, or wrist.
2.) Ulnar nerve entrapment is the second most prevalent compression neuropathy with which patients present. Depending on which nerve fibers are compromised, patients may have weakness in adduction of the fingers. The lumbricals are the major contributors to flexion at the metacarpophalangeal joints as well as extension at the DIP and PIP joints; however, the interossei also play a minor role in these movements.
3.) A late manifestation of ulnar nerve injury, the ulnar Claw hand[3] deformity is caused by weakness of the third and fourth lumbricals.
FAQ
A pair of hand intrinsic muscles that are situated in between the metacarpals are called the palmar interossei. They are made up of four palmar muscles that abduct fingers, and occasionally three. Additionally, the flexion of the metacarpophalangeal joints and the extension of the interphalangeal joints are supported by the palmar interossei.
The fingers are adducted toward the middle finger by the palmar interosseous muscles. The dorsal interossei, on the other hand, abduct the fingers away from the middle finger.
Along with the dorsal interossei muscles, the palmar interossei, also known as volar, are three small, unipennate muscles located on the palmar surface of the hand. The spaces between the metacarpal bones are occupied by these. The little, ring, and index fingers are joined to these.
The lateral base of the second phalanx and the extensor hood of the second digit are where the first dorsal interosseous muscle inserts after starting on the neighboring surfaces of the first and second metacarpal bones.
There is no palmar interosseous muscle in the third finger.
The ulnar nerve’s deep branch supplies all of the interossei. By holding a card between two fingers and asking the patient to hold it firmly, one can test the interossei and therefore the ulnar nerve. Failure to do so suggests muscle weakness or paralysis.