
Spinal Cord
Table of Contents
What is the spinal cord?
~the spinal cord is the lower elongated, cylindrical part of the CNS. It occupies the upper two-thirds of the vertebral canal. It extends from the level of the upper border of the atlas to the lower border of vertebra L1 or the upper border of vertebra L2.

~it is about 45 cm long. The lower end is conical and is called the Conu medullaris.
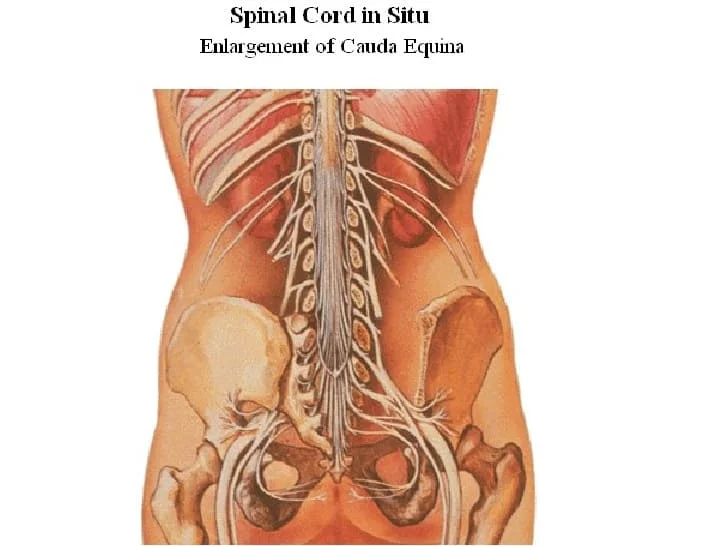
~the apex of the conus is continued down as the filum terminale.
~along its length, the cord presents two thickening, the cervical and lumbar enlargements, which give rise to large nerves for the limbs.

~ The spinal cord gives off 31 pairs of spinal nerves.
Meningeal layers around the spinal cord:-
~duramater S2
~arachnoidmater S2
~piamater L1
~filum terminale
~linea splendens
~ligamenta denticulata
spinal nerves & spinal segments:-
~gives off 31 pairs of nerves
~C8 T12 L5 S5 CO1
~Cervical & lumbar enlargements
~cauda equina
Gray matter:
~H-shaped pillar with anterior & posterior gray matter horns.
~united by the gray commissure containing the central canal.
~lateral gray column (horn)present in thoracic & upper lumbar segments.
~amount of gray matter related to the amount of muscle innervated.
~consists of nerve cells, neuroglia, blood vessels.
nerve cells in the anterior gray columns:
~large & multipolar
~axons pass out in the anterior nerve roots as efferents.
~ Smaller nerve cells are multipolar.
~axons pass out in anterior roots as efferents.
nerve cells in the posterior gray columns.
~4 nerve cell groups:-
~substania gelatinosa:-
~situated at the apex.
~throughout the length of the spinal cord.
~composed mainly of Golgi-type || neurons.
~ receives afferent fibers concerning pain, temperature & touch from the posterior root.
Nucleus proprius:
~anterior to substania gelatinosa.
~present throughout the length of spinal cord.
~main bulk of cells in posterior gray column.
~recevies fibers from posterior white column that are assoc with proprioception ,2-point discrimination,vibration.
Nucleus dorasalis:
~base of posterior column
~C8-L3/L4
~associated with proprioceptive endings.(neuromuscular spindles & tendon spindles)
Visceral afferent nucleus:-
~lateral to nucleus dorsalis.
~T1-L3
~receives visceral afferent info
Nerve cells in the lateral gray columns.
~formed by the intermediolateral group of cells.
~T1-L2/L3
~cells give rise to preganglionic sympathetic fibers.
~in S2, S3, S4, they give rise to preganglionic parasympathetic fibers.
The gray commissure & central canal:-
~connects the gray on each side.
~central canal in the centre
~posterior gray commissure
~anterior gray commissure
~ central canal present throughout
~superiorly continuous with the central canal of medulla oblongata
~inferiorly, expands as the terminal ventricle
~terminates within the root of the filum terminale.
White matter:-
~ divided into:
~anterior white column
~posterior white coumn
~lateral white column
~consists of nerve fibers,neurolgia, blood vessels
~white due to myelinated fibers.
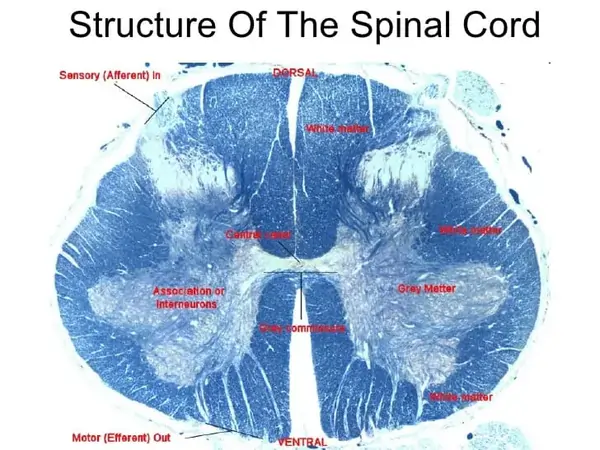
Internal structure:
~When seen in transverse section, the grey matter of the spinal cord forms an H-shaped mass. In each half of the cord, the grey matter is divisible into
1.the anterior grey column(or horn)
2.the posterior grey column(or horn)
~in some parts of the spinal cord a small lateral grey column is also present.
~the grey matter of the right and left halves of the spinal cord is connected across the midline by the grey commissure which is traversed by the central canal.
~the white matter of the spinal cord is divisible into right and left halves,in front by a deep anterior median fissure and behind by the posterior median septum.
~in each half the white matter is divided into:-
1.the posterior white column or posterior funiculus.
2.the lateral white column or lateral funculus nd
3.the anterior white column or anterior funiculus.
~the white matter of the right and left sides is continuous across the midline through the white commissure which lies anterior to the grey commissure.
~the spinal cord gives attachment ,on either side,to a series of spinal nerves.
~each spinal nerve arises by two roots:-
1.anterior (or ventral)
2.posterior(or dorsal)
~each root is made up of a number of rootlets.the length of the spinal cord giving origin to the rootlets for one spinal nerve constitutes one spinal segment.
~as the spinal cord is much shorter than the length of the vertebral column the spinal segments do not lie opposite the corresponding vertebrae.
~in estimating the position of a spinal segment in relation to the surface of the body it is important to remember that a vertebral spine is always lower than the corresponding spinal segment.
~as a rough guide it may be stated that in the cervical region there is a difference of one segment,in the upper thoracic region there is a difference of two segment ,and in the lower thoracic region there is a difference of three segments.
Tracts of the spinal cord:
~A collection of nerve fibers that connects two masses of grey matter within the central nervous system is called a tract.tracts may be ascending or descending.
~they are usually named after the masses of grey matter connected by them.some tracts are called fasciculi or lemnisci.
*Lateral spinothalamic tract:-
~Pain & T
*Anterior spinothalamic tract:-
~Light(crude) touch & pressure
*Fasciculus cuneatus
*Fasciculus gracilis
~discriminatory touch,vibration,info from muscles & joints.
*Anterior spinocerebellar tract
*Posterior spinocerebellar tract
~unconscious info from muscles,joints,skin,sub cut

*Spinotectal tract:-
~spinovisual reflexes
*spinoreticular tract:-
~info from muscles, joints & skin to the reticular formation
*spino-olivary tract:-
~indirect pathway to cerebellum
*Lateral spinothalamic tract:-
~pain & temp pathways
*1st order neurons:-
*pain conducted by A type fibers & C type fibers
*2nd order neurons:-
~deccussate to the opposite side
~ends in thalamus(ventral posterolateral nucleus)
*3rd order neurons:-
~ends in sensory area in postcentral gyrus
*Anterior spinothalamic tract:-
~light (crude) touch & pressure pathways
*Posterior white column:-
~discriminative touch,vibratory sense,consious muscle joint sense(conscious proprioception)
*Posterior spinocerebellar tract:-
~muscle joint sense pathways to cerebellum.
~unconscious proprioception
~muscle joint info from muscle spindles,GTO,joint receptors of the trunk & lower limbs.
~info is used by the cerebellum in the coordination of movements & maintenance of posture.
*Anterior spinocerebellar tract:-
~majority of 2nd order neurons cross to the opposite side.
~enter cerebellum through superior cerebellar peduncle.
~info from trunk ,upper & lower limbs.
~also carries info from skin & subcut tissue.
*Descending tracts:-
~upper motor neurons
~lower motor neurons
~corticospinal tracts:-
~concerned with voluntary,discrete,skilled movements.
*Reticulospinal tract:-
~facilitates or inhibits voluntary movement or reflex activity.
*Tectospinal tract:-
~reflex postural movements in response to visual stimuli.
*Rubrospinal tract:-
~fascilitates activity of flexor muscles & inhibits activity of extensor muscles.
*Vestibulospinal tract:-
~fascilitates extensor muscles,inhibits flexor muscles.
Blood supply:
*Arteries of the spinal cord:
1.anterior spinal artery
2.posterior spinal artery
3.segmental spinal arteries
*Anterior spinal artery:-
~formed by the union of 2 arteries.
~from vertebral artery
~supply anterior 2/3 of spinal cord.
*Posterior spinal arteries:-
~arises from vertebral artery or posterior inferior cerebellar arteries(PICA)
~Descend close to the posterior roots.
~supply posterior 1/3 of spinal cord.
*Segmental spinal arteries:-
~Branches of arteries outside the vertebral column.
~gives off the anterior & posterior radicular arteries.
~great anterior medullary artery of adamkiewicz.
~arise from lateral intercostal artery or lumbar artery at any level from T8-L3
*main source of blood is the vertebral arteries…cervical
~radicular arteries ..spinal branch of vertebral ,asc cervical,deep cervical ,inercostal,lumbar and sacral art
~arteria radicularis magna

*Distribution of blood supply:-
~radicular art:-grey & white matter
~anterior spinal :-ant two-third ventral grey matter, part of dorsal grey matter,ant and lat feniculi
~posterior spinal:-post one third posterior horn and posterior feniculus

Meninges:
*Dura mater:-
~dense,strong fibrous membrane.
~encloses the spinla cord & cauda equina
~continous above with the meningeal layer of dura covering the brain.
~ends at the level of S2.
~separated from the wall of the vertebral canal by the extradural space
~contains loose areolar tissue & internal vertebral venous space
*Arachnoid mater:-
~delicate impermeable membrane.
~lies between pia and dura mater.
~separated from pia mater by subarchanoid space.
~continous above with archanoid mater covering the brain.
~ends on filum terminale at level of S2.
*Pia mater:-
~vascular membrane
~closely covers spinal cord
~thickened on either side between nerve roots to form the ligamentum denticulatum
Clinical importance:
*Spinal shock:
~follows acute severe damage to the spinal cord.
~all cord functions below the level of the lesion become depressed lost.
~sensory impairment and flaccid paralysis occur.
~segmental spinal reflexes are depressed
~persists for less than 24 hours (may be as long as 1-4 weeks)
*Poliomyelitis:
~acute viral infection of the neurones of anterior gray column.
~motor nuclei of cranial nerves.
~death of motor neurons cells-paralysis & wasting of muscles.
~muscles of lower limb more often affected.
*Spinal cord pathology:
*Vertebral cause:-
1.trauma
2.disc prolapse
3.tumor-primary,eg-MM,secondary-eg.breast,thyroid,prostate,bronchus
4.spinal TB-(potts diease)
*Meningeal cause:-
1.epidural abcess
2.tumor-meningioma,neurofibroma,lymphoma,leukaemia
*Spinal cord itself:-
*Developmental:-
~syringomyelia
~meningomyelocoele
~tetherd cord syndrome
*Degenerative:-
~MND
~FA
~SCD
~HSP
*Demyelinating/inflammatory:-
~transverse myelitis
~multiple sclerosis
~neuromyelitis optica
*Infective:-
~bacterial-TB,Syphilis
~viral-EBV,polio,HIV,VZV,HSV
~parasitic-schistosomiasis,toxoplasmosis
*Deficiency:-
~vitamin B12 Deficiency
~vitamin E deficiency
~copper deficiency
~lathyrism
*Vascular:-
~vasculitis
~infraction
~haemorhage
~AVM
*Physcial agents:-
~radiation
~lightening injury
*Paraneoplastic
Localization of spinal cord diease:–
~presence of horizontally defined level below which there will be impairment of sensory,motor,and autonomic function.
*Cervical cord:-
~above C5-spastic qaudriplegia,and diaphgram weakness
~C5-T1:-(qaudriplegia,(LMN signs and segmental sensory loss in the arms & UMN signs in the legs)& respiratory(intercostal) muscle weakness.
~at C5-C6:-loss of power & reflex of biceps
~at C7:-weakness in fingers & wrist extensors & triceps.
~at C8:-finger & Wrist flexion are impaired.
~horners syndrome may accompany
*Thoracic cord:-
~spastic paraplegia with a sensory level on the trunk.
~bowel & bladder involvement
~abdominal reflex(T8-T12)lost above T8 lesion
(segmental lesion T8-T9:above the umbilicus)
(T10-T12:Below the umbilicus)
*Lumbar cord:-
~L2-L4:-
weakness of flexion & adduction of thigh
weakness in leg extension at knee
absent knee jerks(L3-L4)
*L5-S1:-
~weakness of foot & ankle and flexion at the knee & extension of the thigh
~absent ankle jerks(S1)
*Sacral cord:-
~saddle anesthesia(S3-S5)
~prominent bowel & bladder dysfunction & impotence.
~absent bulbocavernous (S2-S4) & anal reflex(S4-S5)
Types of spinal cord lesions:
*complete or transverse lesion
*Incomplete lesion:-
~anterior cord syndrome
~posterior cord syndrome
~hemi cord syndrome
~central cord syndrome
~foramen magnum syndrome
~conus medullaris syndrome
~cauda equina syndrome
*Complete cord transection syndrome:-
~bilateral spastic(paraparesis/quadriparasis)
~bilateral loss of all moodalities of sensation
~bowel & bladder dysfunction
~LMN feature at the level of lesion
~cause:-trauma,vasculitis
*Brown sequard syndrome:-
*Anterior cord syndrome:-
*Posterior cord syndrome:-
*Central cord syndrome:-
*Foramen magnum syndrome:-
*C/F:-
~neck pain-radiating to shoulder
~occipital H/A
~variable sensory loss
~weakness & wasting of hand & neck muscles
~qaudriparesis(round the clock)
*Cause:-
~compressive lesion(meningioma,neurofibroma)in the region of foramen magnum
*Spinal shock syndrome:-
~this clinical condition follows acute severe damage to the cord.
~all cord function below the level of lesion becomes depressed or lost.
~usually last less than 24 hrs bt may last for 4-6 weeks.
~on recovery:-reflex-power-tone may regain this fashion
~5-10% patients may not recover from spinal shock.
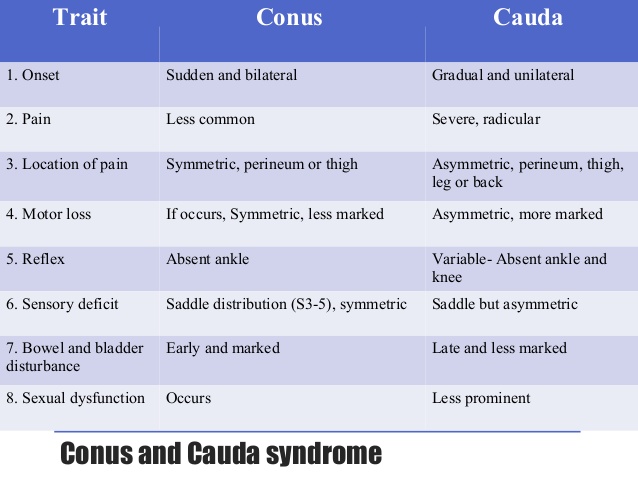
*Conus medullaris syndrome:-
~bilateral saddle anesthesia
~prominent bowel & bladder dysfunction(urinary retention & anal incontinence)
~impotence
~absent anal reflex
~radicular low back pain
~asymmetrical lower limb weakness & sensory loss
~variable areflexia
~relative sparing of bowel & bladder
~planter may be flexor or absent
*cause:-
~disc prolapse
~tumor
~trauma
28 Comments