CLUB FOOT (Congenital talipas equino Varus): Physiotherapy Treatment
Club foot’ also called Congenital Talipes Equino Varus (CTEV) is a rather vague term that has been used to describe a number of different foot-related abnormalities, but over the years it has come to be synonymous with the most common congenital foot deformity mainly CTEV. It rarely occurs mostly once in every 1000 live births.
Table of Contents
Relevant Anatomy
The joints of the foot are: The ankle joint between the talus and the tibia;
- the subtalar joint between the calcaneum and the talus ;
- the talo-navicular joint; and
- the calcaneo-cuboid joint
- the foot is often divided into hindfoot, midfoot and forefoot.
- The hindfoot contain talo-calcaneal (subtalar) and calcaneo-cuboid joints. Midfoot talo-navicular and naviculo-cuneiform joints.The forefoot contains cuneiform-metatarsal and other joints beyond it.
- The ligament related to etiology of club foot are :
- Deltoid ligament:deltoid ligament is a medial collateral ligament of the ankle. It contain superficial and a deep component.
- Spring ligament: This is a ligament join anterior end of the calcaneum to the navicular.
- Interosseous ligament: This ligament lopcated between the talus and calcaneum.
- Capsular ligaments: capsule of the talo-navicular, naviculo-cuneiform, and cuneiform- metatarsal joints, termed as the capsular ligaments, are important structures in pathology of CTEV.
- Planter ligament : these are ligament extendind from the planter surface of the calcaneum to the foot, giving rise to the longitudinal arch of the foot.
- Tendons related to the pathology of clubfoot are those on the medial side of the foot. The tendon immediately run behind the medial malleolus is that of the tibialis posterior. flexor digitorum longus tendon posteriorly, posterior tibial artery and nerve, and flexor hallucis longus tendon. The tibialis posterior tendon has inserted on the navicular bone. This is the most important muscle related to pathology of clubfoot.
- Nomenclature:
- Equinus: In this deformity the foot is fixed in plantar-flexion.
- Calcaneus (reverse of equinus): In this deformity the foot is fixed in dorsiflexion.
- Varus: in this deformity the foot is inverted and adducted at the mid-tarsal joints so that the sole ‘faces’ inwards.
- Valgus: In this deformity the foot is everted and abducted at the mid-tarsal joints so that the sole ‘faces’ outwards.
- Cavus: in this deformity the logitudinal arch of the foot is exaggerated.
- Planus: in this deformity the longitudinal arch is flattened.
- Splay: in this deformity the transverse arch is flattened.
- Aetiology:
- In the vast majority of cases, aetiology is unknown, hence its called idiopathic. In others, the so called secondary clubfoot, some underlying cause such as arthrogryposis multiplex congenita (AMC) can be found. Idiopathic clubfoot: Aetiology of club foot are Following ,
- a) Mechanical theory: The raised intrauterine pressure forces the foot against the wall of the uterus which causes foot deformity.
- b) Ischaemic theory: Ischaemia of the calf muscles during intrauterine life, due to some unknown factor, results in contractures, which causes to foot deformities.
- c) Genetic theory: Some genetically related disturbances in the development of the foot causes foot deformity. Secondary clubfoot: Following are the cause of secondary clubfoot:
- a) Paralytic disorders: In case muscle are imbalance i.e., the invertors and plantar flexors are more stronger than the evertors and dorsiflexors, an equino-varus deformity will develop. This occurs in paralytic disorder for ex., myelodysplasia and Freidreich’s ataxia ,polio , spina bifida, .
- b) Arthrogryposis multiplex congenita (AMC): In this desorder muscles development are defective.the muscles are fibrotic and its causes foot defoemities.
- Pathoanatomy
- All the tissues of the foot for example the bones, joints, ligaments and muscles have developmental abnormality.
- Bones:In this deformity Bones of the foot are smaller than normal. talus neck is angulated so that the head of the
- talus faces downwards and medially. Calcaneum is small, and concave medially.
- Joints: Deformities occur because of malpositioning of different joints:
- Equinus deformity firstly occurs at the ankle joint. Other tarsal joints then other tarsal joint are includes.
- Inversion deformity occurs firsty at the subtalar joint. in inverted calcaneum whole foot faces medially.
- Forefoot adduction deformity occurs at the mid-tarsal joints, most common at talo-navicular joint.
- Forefoot cavus deformity is the result of increase the arch of the foot at the mid-tarsal joints.Muscles and tendons: Muscles of the calf are less develope.
- the following muscles–tendon units are contracted:
- Posteriorly – Tendoachilles
- Medially –
- Tibialis posterior
- Flexor digitorum longus
- Flexor hallucis longus
- Capsule and ligaments: All the ligament structures on the postero-medial side of the foot are shortened.Following are some of others structures like;
- In Posterior –
- Posterior capsule of the ankle joint
- Posterior capsule of the subtalar joint
- Posterior talo-fibular and calcaneo-fibular ligaments
- In Medial –
- Talo-navicular ligament
- Spring ligament
- Deltoid ligament
- In Plantar Plantar fascia
- Plantar ligaments
- Others Interosseous ligament between the calcaneums and talus
- Skin: The skin develops adaptable shortening on the medial side of the sole. There are deep creases onthe medial side present. There are also presents of dimples on the lateral aspect of the ankle and midfoot.
- Secondary changes: These changes occur in the foot if the child starts walking on the foot with deformity.
- Weight bearing may causes exaggerates the deformity.
- Callosities and bursae may develop over the bony prominences on the lateral side of the foot.
Symptoms of Club foot:
- In foot examination, a general examination should be carried out to detect related malformations in other parts of the body.Foot examination: in foot examination Normally, the foot of a newborn child are passivaly dorsiflexed until the dorsum touches the anterior aspect of the tibia This is a very good screening test for detecting the milder variety of CTEV. The more classic one will may have the following findings:
- may present Bilateral foot deformity in 60 per cent cases.
- Size of the foot smaller than normal(in unilateral cases)
- Foot is in equinus, varus and adduction position. This can be confirmed by the inability to bring the foot in the opposite direction. In late cases, in addition, cavus(the londitudinal arch of the foot if exaggerated) of the foot may also be present.
- Heel is small in size; the calcaneum may be felt with to much difficulty.
- Deep skin creases on the back of the heel is also present and on the medial side of the sole.
- Bony prominences also felt on the lateral side of the foot, the head of the talus and lateral malleolus.
- Outer side of the foot is slight convex. There are also presence of dimples on the outer aspect of the ankle.
- On attempted correction, we can feel the tight structures posteriorly (tendoachilles) and plantar-wards (plantar fascia).
- A child presenting late may have callosities over the lateral aspect of deformed foot. The calf muscles are atrophy.
- Presenting complaints: the history dates back to birth, a child with CTEV may present some time after birth occures, often as late as adulthood.
- Following are some of the common presentations are;
- a) Detected at birth: At places where delivery is directed by trained medical Doctor, CTEV is detected at the time of routine screening of newborns to check any congenital mal-formations. At times, the deformity is not that prominant, the so-called postural equino-varus.
- b) Brought during early infancy: At places where delivery is direct at primary health centres, the child is may brought to the hospital around the age of 3-6 weeks.
- c) Brought during late infancy and early childhood: In these cases, the child has received treatment elsewhere, or the deformity has might recurred, or it has never been corrected.
- Unfortunately, in developing countries, a large number of CTEV cases report to the hospital late.
- d) Brought during late childhood: It is not common in developing countries to have a grown up child, or sometimes an adult with CTEV, reporting to the hospital for the first time. Ignorance, poverty and Uneducation are generally the reasons for such late presentations.
Examination:
- General examination: It is aimed at finding an underlying cause of the foot deformity as discussed onA patient of remaining polio may present with equino-varus deformity, which may mimicclubfoot, but there will be may present of paralysis of some other part of the limb. Presence of sensory deficit pointsto an underlying neurological cause. The presence of deformities at other joints may indicate possiblearthrogryposis multiplex congenita (AMC).
Diagnosis:
- This is easy in cases presenting soon after birth of baby. In those presenting late, secondary causes ofCTEV deformity must be excludedX-rays of the foot are done (antero-posterior and lateral view) with the foot in whatevercorrected position possible. The talo-calcaneal angles*, in both, AP and lateral views, in a patient with normalfoot are more than 35 degree , but in CTEV case these are reduced. X-rays are used by some as a method of baseline documentation of the deformities and a method for assessment of correction of deformity after treatment.
Treatment of Club foot:
- Method Of Correction Of Deformity:
- A foot deformity can be corrected by operative or non-operative methods
- .
- Non-operative methods:
- Following are the non-operative methods for correcting deformities:
- a) Manipulation alone: In a newborn, the mother is taught to manipulate the foot after every feed to baby.
- The foot is dorsiflexed and everted . While manipulating, sufficient pressure applied by the person so as to blanch her own fingers. This pressure should be maintained for approx 5 seconds, and this is repeated several times, over a period of roughly 5 minutes. Minor deformities of foot are usually corrected by this method alone. For major deformities of foot, further treatment by corrective plaster casts is required.
- b) Manipulation and PoP: In this method, the surgeon manipulates the deformed foot after sedating the child. The foot is held in the corrected position with plaster casts. There are two philosophies of treatment of clubfoot present : Kite’s and Ponsetti’s.
- Kite’s philosophy: This has been a popular method for over 40 years for foot deformity. The foot is treated by manipulation and PoP, starting at the age of 1 month. The deformities are corrected successfully. Adduction deformity of foot is corrected first followed by inversion deformity and then equinus deformity. A below-knee pop cast is usually sufficient. The casts are changed in every 2 weeks, and are continued until it is possible to ‘overcorrect’ all the foot deformities. Once this happens, the foot is kept in a suitable maintenance device. By this method, correction is may achieved in 30% of cases, over a period of 6-9 months. The rest caseneed surgical correction.
- Ponsetti’s philosophy: Ponsetti’s philosophy is based on proper understanding of the pathoanatomy of the foot with CTEV. By Ponsetti, the calcaneo-cuboid-navicular complex is internally rotated under the plantarflexion of talus, Hence, the deformity can be corrected by gradually stretching the tight structures. This can be done by putting thumb pressure over the head of talus. after doing this, the calcaneo-cuboid-navicular complex is externally rotated under the head of talas. Treatment can be started within 1st week of life. The cavus aspect of the foot deformity is corrected first, followed by the adduction,and then varus and lastly equinus. After every manipulation, an above-knee PoP cast should be applied, which we have to changed every 5-7 days. It is possible to correct all components of the deformity within 6 weeks. The Planterflexed foot deformity in CTEV sometimes remains undercorrected, and can be treated by percutaneous tenotomy of tendoachilles Tendon. The cut tendoachilles regenerates spontaneously.
- Operative methods:
- In case of more severe foot deformities, which are not corrected by non operative method , operative method is required. Soft tissue release operations may be sufficient in younger children who is more than 3 year, but operation of bone are required in older children. The following operations are performed in CTEV.
- a) Postero-medial soft tissue release (PMSTR): Posterro medial soft tiissue release operation consists of releasing the tight soft tissue structures like tendons, ligaments, capsule etc. on the posterior and medial side of the deformed foot. This operation can be performed in younger children. In case of older children, an further bony procedure is required. The following structures are generally released in CTEV.
- On The Posterior Side:
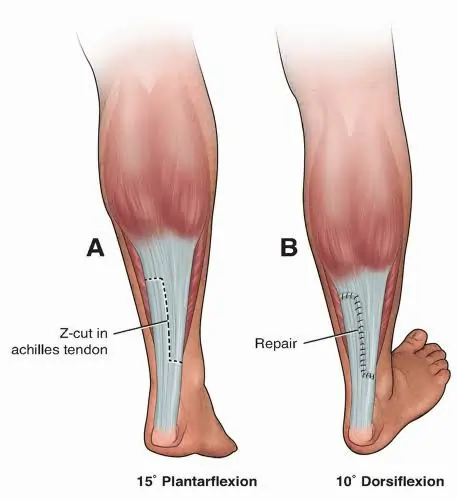
- Lengthening of the tendoachilles by Z-plasty .
- Release of the posterior capsules of the ankle and subtalar joints needed.
- Release of posterior talo-fibular and calcaneo-fibular ligaments.
- On The Medial Side:
- Lengthening of 3 tendons* i.e., tibialis posterior, flexor digitorum longus and flexor hallucis longus. In addition, their contracted thickened sheaths are excised.
- Release of 3 ligaments i.e., talo-navicular ligament, superficial part of the deltoid ligament and the spring ligament.
- Release of more 3 structures is needed in severe cases of CTEV. These are the interosseous talo-calcaneal ligament, capsules of the naviculo- cuneiform and cuneiform-first metatarsal joints.
- On The Plantar Side:
- Plantar fascia release.
- Release of the short flexors of the toes which is flexor digitorum brevis and abductor hallucis from their origin on the calcaneum.
- b) Limited soft tissue release:
- In some cases, the deformed foot remains partially corrected after non operative treatment, and only limited soft tissue release may be sufficient as shown below:
- For equinus alone a posterior release needed
- For adduction alone a medial release needed
- For cavus alone a plantar release needed
- c) Tendon transfers:
- In some cases of CTEV, the tibialis anterior and tibialis posterior the invertors of the deformed foot may cause a deforming force against the weak peroneus longes and peroneus brevis. This muscle imbalance may be corrected by transfering the tibialis anterior to the outer side of the deformed foot, where it acts as an everter of foot. Minimum age for transfers of tendon is 5 years.
- d) Dwyer’s osteotomy: Dwyer’s osteotomy is an open-wedge osteotomy of the calcaneum, performed to correct varus of the heel. Minimum age at which Dwyer’s osteotomy procedure we can performed is around 3 years, as prior to this the calcaneum is mainly cartilaginous. Some prefer a closed-wedge osteotomy on the lateral side calcaneum.
- e) Dilwyn Evan’s procedure:
- Dilwyn Evan’s procedure consists of a thorough release of soft tissue with calcaneo-cuboid fusion . It is used for a neglected or recurred clubfoot in children with age between 4-8 years. With fusion of the calcaneo- cuboid joint, the lateral side of the foot does not grow as much as the medial side, this causes gradual correction of the deformity.
- f) Wedge tarsectomy:
- Wedge tarsectomy performed by removing a wedge of the bones from the mid-tarsal area. The wedge of bone is cut with base on the dorso-lateral side. Once the wedge is removedt he foot can be brought to normal position. This operation is performed for neglected clubfeet with child between the age of 8-11 years.

- g) Triple arthrodesis:
- Triple arthrodesis consists of the fusion of three subtalar, calcaneo-cuboid and talo-navicular joints of the foot, after taking suitable wedges to correct the foot deformity.Triple arthrodesis is performed after 12 years of age, because before this the bones of the foot are cartilaginous and it is to difficult to achieve fusion. talo- navicular joint fusion is most difficult to achieve in Triple arthrodesis.
- h) Ilizarov’s technique:
- Using the principles of Ilizarov’s technique, different components of the foot deformity are corrected by gradual stretching, using an external fixator. Once correction is achieved, it is maintained by POP casts. Ilizarov’s technique isused in neglected clubfeet, and in those case in which it has recurred after previous operation.
- Methods Of Maintenance Of The Correction :
- when Correction once achieved, is maintained by the following methods:
- a) CTEV splints: Congenital talipes equino varus splints made of plastic, moulded in such a way that when tied with straps,which keeps the deformed foot in corrected position.
- b) Denis-Brown splint (DB splint): denis Brown splint used to hold the deformed foot in the corrected position. It is used whole the day before the child starts walking.
- c) CTEV shoes: CTEV shoes are modified shoes, used when a child starts walking. The following modifications are made in the CTEV shoe
- Straight inner border used to prevent forefoot adduction.
- Outer shoe raise used to prevent foot inversion.
- shoes without heel used to prevent equinus.
- CTEV shoes are used until the child is 5 years old.
- Plan Of Treatment :
- Most cases which are treated early, respond when non-operative methods. Operative methods may be indicated in the following cases:
- a) A child who does not respond without operative treatment (resistant clubfeet): These feet are generally severely deformed, ‘chubby’ orrelated with underlying arthrogryposis multiplex congenita (AMC).
- b) A child whose foot deformities have recurred : This usually happens if correction is not maintained. The first deformity to recur is the equinus (planterflexed).
- c) A child who has presented late or has not been sufficiently treated (neglected clubfeet).
- Physiotherapy Treatment :
- Exercise should be begin as soon as your child’s surgeon recommends it. Physiotherapy treatment applied to the patient either treatment is surgical or non-surgical.
- Goal :
- Increased Range of motion
- Prevent weakness of muscles
- prevent Tightness and contracture of muscles
- increased strength and endurance of muscles
- Treatment :

- Passive exercise of Hip,knee,and ankle joints
- HIP Joint
- Flexion
- Extention
- Abduction
- Adduction
- Internal Rotation
- Exeternal Rotation
- Knee Joint
- Flextion
- Extention
- Ankle Joint
- Dorsiflexion
- PlanterFlexion
- Inversion
- Eversion
- Stretching exercise should be given to the muscles to align foot.
- Mobilization techniques also helps to reduce pain.
- To improve strength of muscles, strengthining exercise should be given.
- we can give Electrical stimulation to strengthen the Dorsiflexors muscles.
- To restore stability, retrain the lower extremity and improve movement techniques and mechanics for example, walking, gait training, running or jumping of the affected lower extremity to reduce stress on the joint surfaces in daily activities.
- Rhythmic and repeated gentle manipulation.
- Strapping and plaster of Paris cast should be given.
- Education and instructions Related to Deformity to the mother and/or parents shpuld be given.
- Modalities including the use of ultrasound, electrical stimulation, ice, cold, laser to Reduced pain and inflammation of the involved joint we can use.
- CTEV Splint :

- CTEV Shoes :