
GUYON’S CANAL SYNDROME
Table of Contents
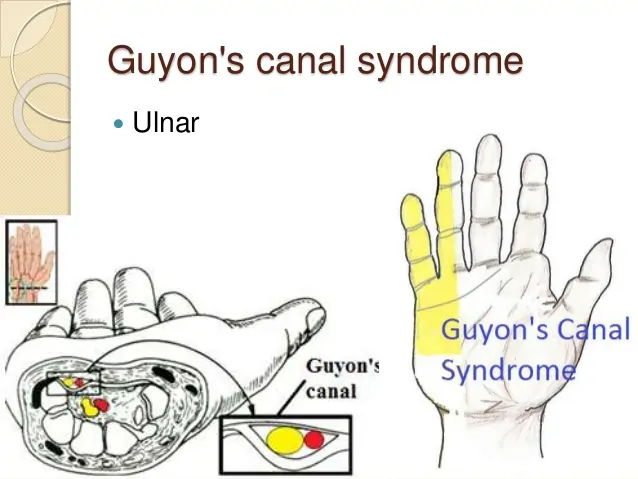
What is Guyon’s Canal Syndrome?
Guyan’s canal syndrome is also known as Ulnar tunnel syndrome & Handlebar palsy. In Guyon’s canal syndrome, there is a compression of the ulnar nerve when it passes through the wrist into the hand through a space called the Guyon’s canal (ulnar tunnel).
Introduction:
- It is a relatively rare peripheral ulnar neuropathy that involves injury to the distal portion of the ulnar nerve as it travels through a narrow anatomic corridor at the wrist.
- Symptoms usually begin with a feeling of pins and needles in the ring and little fingers before progressing to a loss of sensation and/or impaired motor function of the intrinsic muscles of the hand
- The clinical presentation can be purely sensory, purely motor, or both depending on the location of the nerve compression
Anatomy:
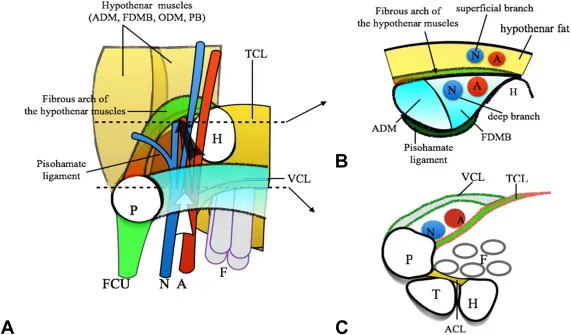
- The Guyon Canal extends between the proximal border of the pisiform bone and distally at the hook of the hamate.
- The ulnar nerve and ulnar artery pass through the Guyon canal as they pass from distal forearm to the hand.
- The boundaries of Guyon canal are:
- Roof: palmar carpal ligament, palmaris brevis and hypothenar connective tissue.
- Floor: transverse carpal ligament, pisohamete ligament, pismetacarpal ligament, flexor digitorum profundus tendons and opponens digiti minimi.
- Medial wall: pisiform, abductor digiti minimi and flexor carpi ulnaris tendon.
- Lateral wall: hook of hamete, transverse carpal ligament and the flexor tendons.
What are the Causes of Guyon Canal Syndrome?

- Injury to the distal ulnar nerve can be due to compression, trauma, inflammation or vascular insufficiency.
- Ganglion cysts, they’re one of the most common causes of Guyon canal syndrome.
- Tumors
- Anatomical anomalies, can be hypertrophic muscle of normal anatomy or unusual location
- Fractures or dislocations (e.g., The hook of hamate Fracture/Displacement)
- Repetitive trauma (e.g., repetitive trauma to the hypothenar by the handlebar in cyclists)
- Carpel tunnel syndrome, it can lead to anatomical changes in the ulnar tunnel leading to functional impairments
- Iatrogenic
- Hypothenar Hammer Syndrome (HHS) is a unique mechanism of ulnar nerve injury secondary to ulnar artery thrombosis or an aneurysm, which results in inflammation and subsequent compression of the ulnar nerve at Guyon canal
What are the Symptoms present in Guyon’s Canal Syndrome?
- Ulnar tunnel syndrome usually produces symptoms in the hands and wrist, especially the little finger and ring finger
- Paraesthesia and tingling affecting the little and ulnar half of ring finger (dorsum of hand is spared in Guyon’s canal syndrome in contradistinction to cubital tunnel syndrome where the ulnar dorsum of the hand is also affected).
- Clawing of ring and little fingers (tend to be worse than cubital tunnel syndrome, the so-called “ulnar paradox”).
- Weakened grasp, pinch
- Abducted posture of the little finger (Wartenberg sign)
- Wasting of hypothenar muscles and guttering of the hand (wasting of interosseous muscles)
Symptoms grades:
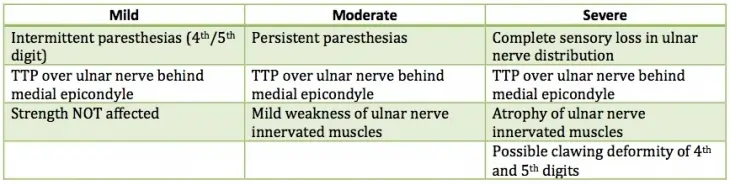
Depend on the severity of symptoms:
- Very mild
- Mild
- Moderate
- Severe
- Very severe
Depend on the Duration of symptoms:
- Acute (within one month)
- Sub-acute (two to three months)
- Chronic (more than three months)
Classification:
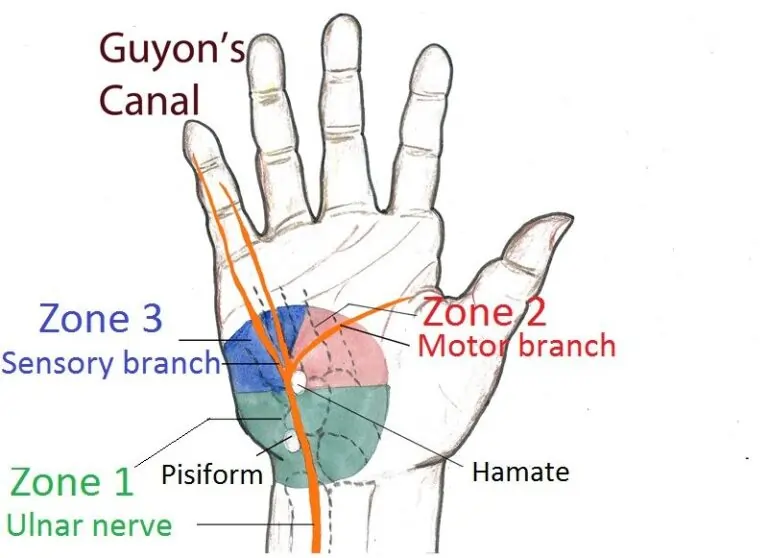
- Ulnar tunnel syndrome may be characterized by the location or zone within the Guyon’s canal at which the ulnar nerve is compressed.
- As the ulnar nerve passes through Guyon’s canal it splits into deep motor branch and superficial sensory branch.
zone 1: proximal to the motor/sensory bifurcation
- Area of the distal portion of the ulnar nerve (main trunk) before it splits into its superficial sensory and deep motor divisions
- Etiologies include hook of hamate fracture/malunion/nonunion, ganglion cysts
- Zone 1 Guyon canal injury to the ulnar nerve results in mixed motor and sensory symptoms
Zone 2 (most commonly affected): distal to motor/sensory bifurcation, and radial to zone 3
- Corresponds to the deep terminal motor branch of the ulnar nerve, if affected, it produces only motor symptoms (e.g. weakness)
- Etiologies include hook of hamate fracture/malunion/nonunion, ganglion cysts
- This deep branch of the ulnar nerve innervates all the interosseous muscles, fourth and fifth lumbricals, hypothenar muscles (opponens digiti minimi, abductor digiti minimi, flexor digiti minimi brevis), and adductor pollicis muscle.
Zone 3: distal to motor/sensory bifurcation, and ulnar to zone 2
- The superficial sensory terminal branch of the ulnar nerve is compromised in this zone producing sensory symptoms only (e.g., numbness and tingling, burning sensation)
- Etiologies include ulnar artery aneurysm and/or thrombosis
Risk factor :

- It has had a previous injury to its wrist
- Performs repetitive tasks with the hands, such as typing
- Are activities or sports that put the wrist under strain
- Uses vibrating tools
Diagnosis:
- Radio graphs in the case of wrist trauma [Radio graphs in the case of wrist trauma].
- CT scan may be necessary to delineate hook of hamate fracture.
- MRI scan is useful to exclude any space-occupying lesion e.g. ganglion.
- Doppler ultrasound is useful to evaluate the flow in the ulnar artery.
- Angiography can be used for the evaluation of ulnar artery aneurysm or thrombosis.
- Nerve conduction studies are useful in confirming the diagnosis and localizing neuropathies.
Physical Examination:

- The first step in physical examination is observation of the hand for clawing.
- Atrophy of the hypothenar or interossei.
- Inability to cross fingers or any masses over the wrist.
- Tenderness over the hook of hamete can indicate fracture.
Special test:
Tinel sign:
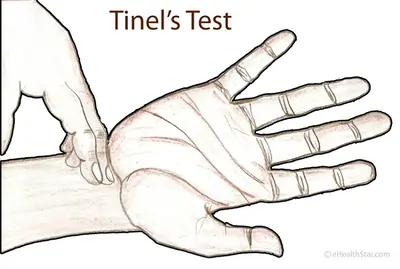
- It involves reproducing symptoms by tapping at the site of suspected nerve compression and can also be used for localization .
- Compromise of the deep motor branch of the ulnar nerve within Guyon canal can result in weakness of the adductor pollicis muscle .
Froment’s sign:
- It observed, when the patient is asked to hold a piece of paper between his thumb and fingers as the examiner tries to pulls it.
- Weakness in adductor polices muscle (supplied by the ulnar nerve) would result in compensatory movement of thumb flexion instead of thumb adduction .
Wartenberg sign:

- When the fifth digit is observed in an over-abducted position at rest, this is known as Wartenberg sign,
- Which can be seen in ulnar nerve palsy as a consequence of denervation of the palmar interossei muscles that are normally responsible for digit adduction.
Allen Test:

- IT IS evaluates the arterial supply of the hand, which is useful when Ulnar Artery Thrombosis is suspected.
Medical treatment:
- On starting phase of patient give to medical treatment
- Anti-inflammatory drugs – NSAIDs
- Cortisone injections.
Conservative treatment:

- Activity modification
- NSAIDS
- Splinting
- In Activity modification such as in cyclists in terms of posture, adjustment of bike and protective equipment.
Surgical treatment:
- The aim of the surgery is to decrease the pressure on the ulnar canal in Guyon’s canal by removing the roof of the Guyon canal or removing the structures compressing the nerve.
Local surgical decompression:
Indications :
- Severe symptoms that have failed nonoperative treatment.
Techniques :
- Release hypothenar muscle origin.
- Decompress ganglion cysts.
- Resect hook of hamate.
- Vascular treatment of ulnar artery thombosis.
- Explore and release all three zones in Guyon’s canal.
Tendon transfers:
Indications :
- Correction of clawed fingers.
- Loss of power pinch.
- Wartenberg sign (abduction of small finger).
Techniques:
Correct claw fingers:
- Possible grafts include ECRL, ECRB, palmaris longus.
- Tendons must pass volar to transverse metacarpal ligament in order to flex the proximal phalanx .
- Attach with either a two or four-tailed graft to the A2 pulley of the ring and small fingers.
Restore power pinch :
- Smith transfer using ECRB or FDS of ring finger.
Restore adduction of small finger:
- Transfer ulnar insertion of EDM to A1 pulley or radial collateral ligament of the small finger.
Carpal tunnel release:
Indications:
- Patients diagnosed with both ulnar tunnel syndrome and CTS.
Physiotherapy Treatment in Guyon’s Canal Syndrome:
After Conservative treatment:
- Ultrasound (US)
- Nerve glide exercise
Nerve glide exercise :
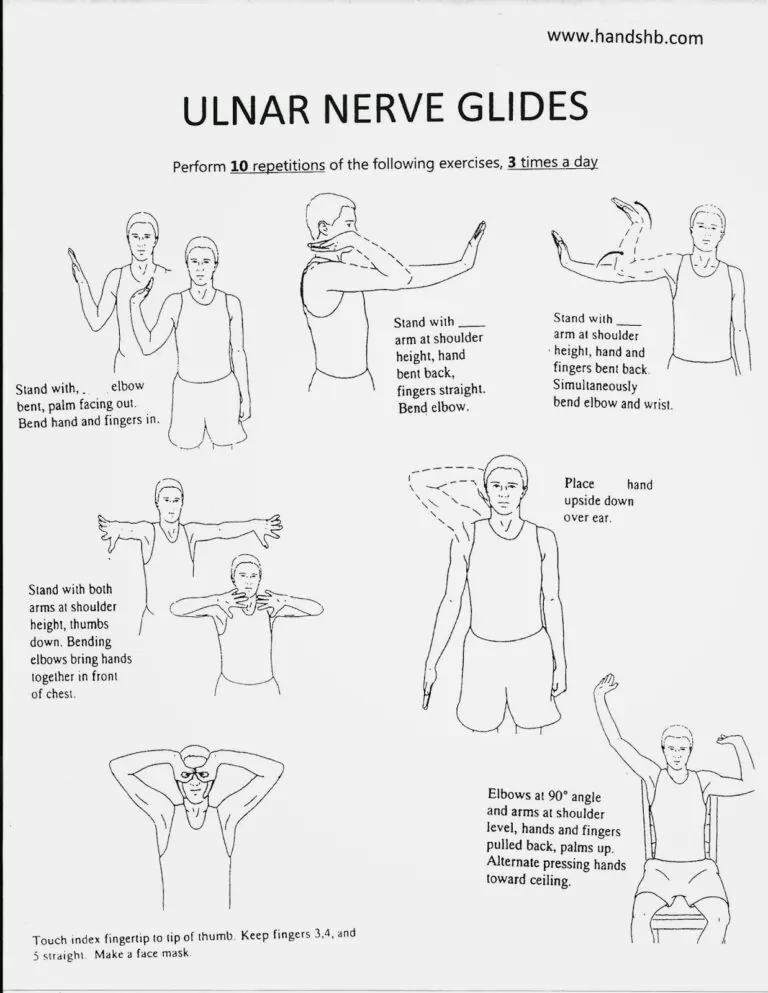
- Wrist extension
- forearm pronation
- elbow flexion,
- glenohumeral lateral rotation
- glenohumeral depression,
- shoulder abduction.
The patient is follow the some instruction:
- To avoid activities that cause repetitive stress at Guyon’s canal such as weight bearing or cycling or modification of the bicycle handlebars.
- Also, to avoid static postures or repetitive movements that places mechanical overload such as prolonged wrist extension.
- The patient is instructed to wear resting hand splint to place the wrist in neutral position.
- The splint should be worn for 1-12 weeks during night time and at day time during aggravating activities.
After surgical treatment:
During the early post-operative period (up to 10-15 days after surgery):
- Advised to patient elevate his hand.
- Provide appropriate rest of the hand.
- Do gradual hand and wrist movements without resistance as tolerated.
- Avoid applying heavy loads on the hand or doing forceful activities.
Post-surgical:
Scar care:
- Apply splint for scar
- Apply massage with use of oil
Edema control :
- Elevated the palm
- Apply massage
- US is given to patient
- Compression bandage given to patient
Hand and wrist mobilization:
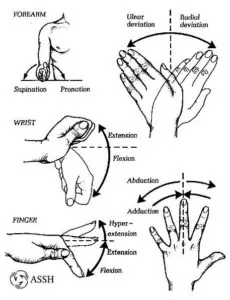
- Hand and wrist movement [ flexion, extension. redial deviation, ulnar deviation ]
- In starting active, then strengthening
Grip strengthening exercise:
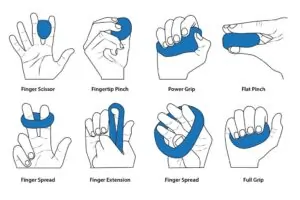
- Squeezing a Tennis or Racket Ball.
- Standing Cable Row With a Towel.
- Rubber-Band Exercise
- Tip to tip , pad to pad , tip to pad exercise with use of paper , manual
Forehead touch exercise.
- Stand straight with arms at the sides
- Raise one hand, so the palm is resting on the forehead
- Hold it here for a few seconds then slowly bring the hand down again
- Repeat the exercise
Hand curl exercise:
- That stretches the ulnar nerve.
- Stand or sit upright with the arm held straight in front of the body with the elbow straight
- Curl the wrist and fingers towards the body
- Then, extend the hand away from the body to feel a stretch in the wrist
- Finally, bend the elbow and raise the hand upwards
- Repeat the exercise
Ulnar nerve Strengthening Exercise:
- Stand straight with your arms at your side.
- Raise the affected arm and rest your palm on your forehead.
- Hold your hand there for a few seconds and then bring your hand down slowly.
- Repeat the exercise a few times a day, gradually increasing the number of repetitions you do in each session.

4 Comments