
Levator Scapulae Muscle
Table of Contents
Levator Scapulae Muscle Anatomy
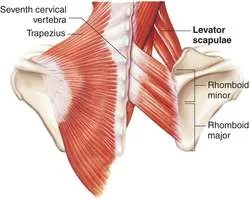
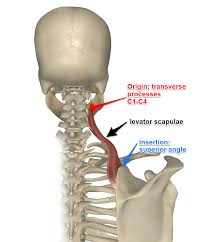
The levator scapulae muscle is a long muscle of the shoulder girdle. It is situated at the back and the side of the neck, and as its name suggests – its main function is to lift the scapula. The position of the muscle defines its supportive role in the vertebral column.
Together with other posterior axial-appendicular muscles, the levator scapulae are capable of extending and laterally flexing the neck as well as inferiorly rotating the glenoid cavity. Another function of the levator scapulae is to link the superior appendicular skeleton with the axial skeleton. Many conditions can affect the levator scapulae, such as fibromyalgia, cervical myofascial pain, Sprengel deformity, snapping scapula syndrome, and levator scapulae syndrome.
Origin
It originates from the posterior tubercles of the transverse processes of C1 to C4.
Insertion
It inserts into the superior part of the medial border of the scapula.
Nerve supply
The dorsal scapular nerve supplies the muscle.
The dorsal scapular nerve (DSN), which arises from the C4 and C5 nerve roots, is usually responsible for innervating the levator scapulae. Additionally, the rhomboids get motor innervation from this nerve. The DSN, which is usually the first nerve branch off the C5 root, originates from the upper brachial plexus and the anterior rami of the C5 root. Cervical nerves (C3, C4) can also innervate through the cervical plexus.
Blood supply
The levator scapulae is supplied by the dorsal scapular artery. Normally, this artery has a small branch that passes laterally to the supraspinatus fossa of the scapula, and in a third of cases, this branch supplies the muscle.
Action
Scapulothoracic joint: Draws scapula superomedially, rotates glenoid cavity inferiorly;
Cervical joints: Lateral flexion of the neck (ipsilateral), an extension of the neck
Function
The main function of the levator scapulae muscle is to elevate and retract the shoulder girdle at the scapulothoracic joint. At the same time, it helps in preventing the depression of the girdle when carrying heavy loads. Additionally, the muscle participates in the stabilization of the scapula and the inferior rotation of the glenoid cavity.
When acting on the cervical joints, unilateral contraction of the muscle produces ipsilateral flexion of the neck, while bilateral contraction contributes to the extension of the neck. The actions of levator scapulae are facilitated by actions of the trapezius, latissimus dorsi, rhomboids, and pectoralis major and minor muscles.
Embryology
The paraxial mesoderm is where the rhomboid major and minor muscles as well as the levator scapulae muscles originate. Fibroblast growth factor (FGF) and Wnt signaling stimulate the formation of these cells in tailbud neuromesodermal progenitors. The anterior (motor) rami of C5 are the source of the dorsal scapular nerve. The spinal cord’s basal plate area gives rise to the anterior root.
Anatomic variations in the subclavian artery may be responsible for supraclavicular brachial plexus blocks that do not work. For upper limb anesthesia and analgesia, physicians execute supraclavicular brachial plexus blocks. In a case report, Kohli et al. describe an ultrasound-visualized variant branch of the subclavian artery that may be the dorsal scapular artery, which passes through the brachial plexus nerve bundle.
Anatomical Variations
The origin and insertion of the levator scapulae have been reported to show anatomic variations. The importance and clinical implications are uncertain.
Levator Scapulae Muscle Exercises
Strengthening exercise
Stand against a wall with a spikey ball placed on your upper back above your scapula (on the levator scapulae muscle). Apply a comfortable pressure (“feel good” pain). Keep the pressure, and move your body up and down to slowly roll the ball along the muscle. You can pause on the tighter spots for up to 30 seconds.

Stretching Exercise:

- Sit on a chair or bench with your feet wide apart and your back and abs slightly tightened.
- Reach behind you with your right hand and grab the edge of the chair. Lean your upper body to the left, keeping your head upright.
- You will feel a light pull in your right shoulder or upper arm.
- Now try to lift your right shoulder toward the ceiling for five seconds. Do not allow your body to move sideways.
- Relax for a couple of seconds and then lean your upper body a little more to the side.
- You have now reached the correct starting position for the stretch.
- Rotate your head 45 degrees to the left. Place your left hand behind your head and gently pull it at an angle toward your knee.
- Stretch the muscle in this manner for 5 to 10 seconds.
- Stop the movement when you feel a slight sting in the right side of your neck. Next, relax the muscle for 5 to 10 seconds.
- Resist by carefully pushing your head backward into your hand. Next, relax the muscle for 5 to 10 seconds.
- Deepen the stretch by slowly pulling your head toward your chest in the direction of your knee until you reach a new ending point.
- Repeat two or three times.
Related pathology
An isolated lesion of the dorsal scapular nerve with a consequent paralysis of the levator scapulae muscle is very rare. The symptoms include “winging” of the scapula (scapula alata), as well as atrophy of both the levator scapulae and rhomboid muscles. As the affected patients may have no clear complaints, the correct diagnosis is often made too late.
Levator scapulae is one muscle of the human body that is prone to stiffening and chronic pain due to false posture in everyday life. Common causes include carrying heavy shoulder bags, permanent lifting of the shoulders while sitting at a desk, and sleeping on one side of the body without proper head support.
Levator scapulae syndrome
Levator scapulae syndrome, or soreness across the upper medial angle of the scapula, is the most typical clinical sign of levator scapulae dysfunction. Despite a wealth of evidence, this illness is frequently ignored. Muscle-stretching activities often exacerbate pain. Constant trigger points, crepitation, and enhanced heat emission are thought to be caused by anatomic variability combined with a bursa that confluences between the scapula, origin serratus anterior, and levator scapulae insertion. Physical therapy and/or local corticosteroid injections are effective forms of treatment.
Snapping Scapula Syndrome
Severe shoulder dysfunction, often known as “washboard syndrome” or snapping scapula syndrome, can manifest as excruciating crepitus or scapulothoracic bursitis. Usually, a persistent injury, overuse, or muscular imbalance that affects the scapulothoracic articulation is the secondary cause of this condition’s manifestation.
Avulsion of the levator scapulae orosseous lesions at the superomedial angle of the scapula as a result of repetitive damage has also been linked to the clinical presentation. Owing to recurring injuries from upper extremity load-bearing tasks and chronic stress, this syndrome may be more common in military personnel. With an 80% success rate, treatment is usually conservative. Arthroscopy bursectomy, with or without partial scapulectomy, is the most successful therapeutic option for patients who do not respond to conservative measures.
Myofascial Pain
Pain that is related to muscles and the fascia that surrounds them is known as cervical myofascial pain, which is a musculoskeletal condition. One of the cervical spine’s most often affected muscles is the levator scapulae. Though its exact cause is unknown, postural mechanics, misuse of the muscles, trauma, or secondary to another pathologic illness like fibromyalgia or zygapophyseal joint arthropathies are major causes of myofascial pain. Localized, regional, or trigger point-characterized cervical myofascial pain is all possible. Trigger points are hypersensitive regions in the muscle that, when stimulated mechanically, can cause pain in the surrounding tissue. Trigger points are often found in the levator scapulae, where fibromyalgia is often diagnosed based on the presence of a painful point in this area.
Trigger points in Levator Scapulae Muscle
Additionally, a significant incidence of active levator scapula trigger points has been recorded in certain situations, particularly those resulting from acute whiplash injuries. A painful insertion site is associated with dysfunction of the upper and middle cervical spines. Patients with Sprengel deformity have varying degrees of levator scapulae atrophy.

3 Comments