
Abdominal Wall
Table of Contents
Introduction:
The abdominal cavity surrounds by the abdominal wall, providing it with flexible coverage and protecting the internal organs from injuries. The abdominal wall is bounded superiorly by the xiphoid process and costal margins, posteriorly by the vertebral column, and inferiorly by the pelvic bones and inguinal ligament.
Parts Of Abdominal Wall
The abdominal wall is divided into two parts:
- anterolateral wall
- posterior abdominal walls
Layers Of Abdominal Wall:
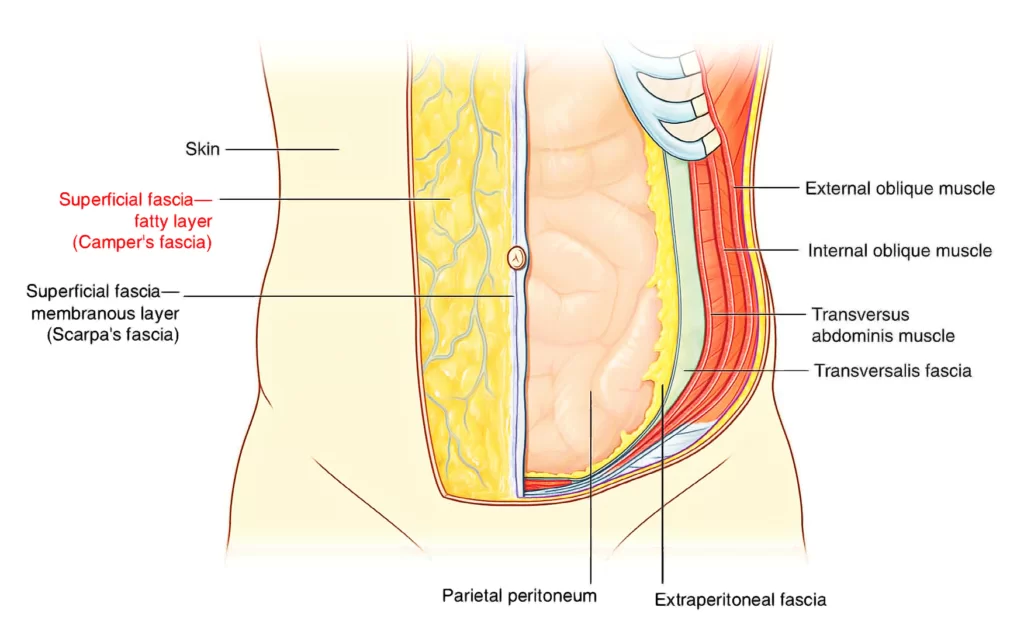
This complex structure contains numerous layers, from superficial to deep
- Skin
- Subcutaneous tissue
- Fascia
- Camper’s fascia – fatty superficial layer.
- Scarpa’s fascia – deep fibrous layer.
- Superficial Abdominal fascia
- Muscle
- External oblique abdominal muscle
- Internal oblique abdominal muscle
- Rectus abdominis
- Transverse abdominal muscle
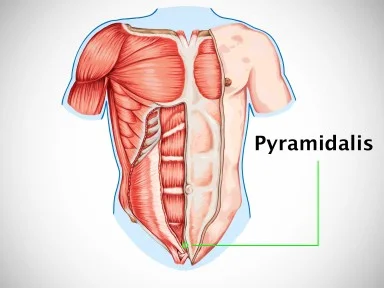
- Pyramidalis muscle
- Transversalis fascia
- Extraperitoneal fat
- Peritoneum
Anterolateral abdominal wall
The anterolateral wall of the abdomen spans the anterior and lateral sides of the abdomen. It can be divided into several topographical areas, which are used to describe the location of abdominal organs and the pain related to them:
Four quadrants are divided by the horizontal transumbilical and vertical median planes. The four resulting areas are known right upper, left upper, right lower, and left lower quadrants.
Nine abdominopelvic regions are divided horizontally by the superior subcostal plane, which passes right under the costal margins of the 10th number ribs, and the inferior intertubercular plane, which connects the tubercles of the iliac crest of the pelvis. Vertically they are divided by the two midclavicular planes which pass through the midpoint of each clavicle and halfway between the pubic symphysis and the anterior superior iliac spine(ASIS). The four planes create nine abdominal regions: hypochondriac (right, left) and epigastric regions superiorly, flanks (right, left) and umbilical region in the middle, groin (right, left), and hypogastric region inferiorly.

Fascia
The most superficial layer of the anterior abdominal wall is the skin. In obese people, pregnant women, and those with abdominal distention, it can contain elongated lines called stretch marks or striae distensae, usually situated in the umbilical regions and hypogastric regions. The superficial fascia is located just under the skin and consists of connective tissue. The anterior abdominal wall, superior to the umbilicus, is similar and continuous to the superficial fascia of the body and is made up mostly of one layer. inferior to the umbilicus, it is divided into two layers:
1)Fatty layer of subcutaneous tissue (Camper’s fascia) (Panniculus adiposus abdominis);
2)The membranous layer of subcutaneous tissue (Scarpa’s fascia) (Stratum membranosum telae subcutanei abdominis)
Superficial Camper’s fascia is a thicker fatty layer that can have a different degree of thickness. For example, it is greatly increased in obese people and very thin in people with low body fat.
Deep Scarpa’s fascia, is a thin and denser membranous layer under the muscle layer of the abdominal wall. Deep Scarpa’s fascia is firmly attached to the linea alba and pubic symphysis and fuses with the fascia lata (deep fascia of the thigh) right below the inguinal ligament.
In men, the Camper’s fascia continues over the penis and blends with the Scarpa’s fascia to make the superficial fascia of the penis. The latter extends further into the scrotum, where it contains smooth muscle fibers and becomes the dartos fascia. Scarpa’s fascia continues into the perineum to form the superficial fascia of the perineum, which is called Colles’ fascia. In the women, it continues into the labia majora and anterior perineum.
Anterolateral abdominal wall Muscles
If we go deeper into the anterolateral abdominal wall, under the superficial fascia we will find the muscular layer. It contains five paired muscles and their respective aponeuroses. The muscles of the anterolateral abdominal wall are divided into two main muscles groups:
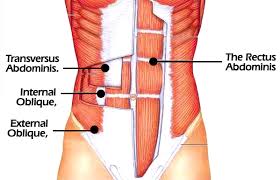
The lateral flat muscle group is located on either side of the abdomen and includes three muscles: external oblique, internal oblique, and transversus abdominis.
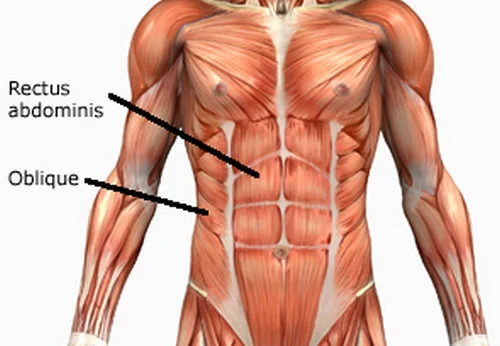
Anterior vertical muscles are located bilaterally to the median fibrous structure called the linea alba. They are called rectus abdominis muscles and pyramidalis muscles.
Lateral abdominal muscles
These flat muscles are part of the tension system of the abdominal wall muscles. Through the abdominal press, they increase the intra-abdominal pressure and thereby support emptying processes for example defecation, micturition, and exhalation (expiratory breathing muscles). Their unilateral contraction results in rotation of the torso.
The external oblique muscle is the outermost muscle, whose fibers run inferior and medially. Right beneath it sits the internal oblique muscle whose fibers run superior and medially. The most profound lateral muscle is the transversus abdominis muscles which consist of horizontal fibers. The transverse fascia is located below the transversus abdominis muscles.
The external oblique is a lateral flat muscle that courses from the 5th to the 12th rib ventromedially until the anterior layer of the rectus sheath. At its origin, it is tightly connected with the serratus anterior muscle and latissimus dorsi muscles. Ventrally the external oblique muscle builds a large aponeurosis which extends medially to the linea alba and caudally to the iliac crest and the pubic bone of the pelvis. Its inferior margin makes the inguinal ligament.
Originating from the thoracolumbar fascia, iliac crest, and iliopectineal arch, the internal oblique inserts cranially at the lower costal cartilages and ventrally at the linea alba. In men, caudal fibers extend to the spermatic cord and merge to make the cremaster muscle. The semilunar lines (linea semilunaris) are formed by the divisions of the internal oblique aponeurosis and correspond with the lateral margins of the rectus abdominis muscles. They extend from the 9th coastal cartilage tips to the pubic tubercle.
The transversus abdominis muscle is the deepest muscle of the three lateral abdominal muscles. transversus abdominis muscle runs from the inner surface of the lower costal cartilages, thoracolumbar fascia, iliopectineal arch, and iliac crest horizontally to the linea alba. Caudal fibers are also get involved in the formation of the cremaster muscle. The anterior abdominal wall from the extraperitoneal fat separates by transversalis fascia. In Posteriorly, the transversalis fascia is continuous with the thoracolumbar fascia.

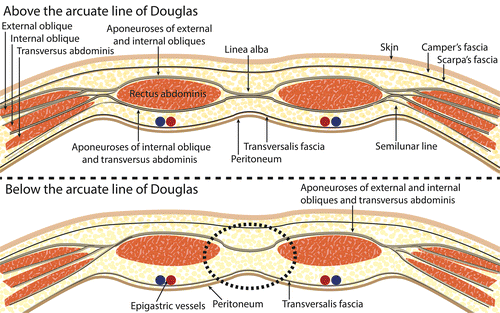
The aponeuroses of these muscles form the rectus sheath, which is divided into anterior layers and posterior layers. The latter is only available in the superior three-quarters of the rectus sheath and its inferior limit is demarcated by the horizontal arcuate line. This is where the inferior epigastric artery and inferior epigastric vein perforate the rectus abdominis. Above the arcuate line, the anterior layer consists of the aponeuroses of the internal oblique and external oblique, while the posterior layer is made up of the aponeuroses of the internal oblique muscles and transversus abdominis muscles. Below the arcuate line, the anterior layer of the rectus sheath is built by the aponeuroses of all three lateral abdominal muscles whereas the posterior layer of the rectus sheath is only covered by the transverse fascia and the peritoneum.
Anterior abdominal wall muscles
The anterior muscle group includes the rectus abdominis muscles and pyramidalis muscles. These are almost completely enveloped by the thick rectus sheath made up of the aponeuroses of the lateral abdominal muscles. The only exception is the posterior side of the lowest fourth of the rectus abdominis muscle, below the arcuate line, which is covered by the only transversalis fascia and parietal peritoneum. Immediately deep into the rectus sheath is the transversalis fascia, under which lie the two deepest layers of the abdominal wall: extraperitoneal fat and peritoneum.
The rectus abdominis is a pair of long, straight muscles that run vertically on either side of the anterior abdominal wall. They are separated by the linea alba. The term rectus abdominis means “straight abdominal” in Latin, which indicates that the muscle fibers run in a straight vertical line through the abdominal region of the body. Each muscle contains a string of four fleshy muscular bodies connected by three narrow bands of tendon known as tendinous intersections. The shape of these segments is often visible through the superficial fascia and skin in those who have low body fat, resulting in a ‘six-pack’ shape.
The pyramidalis muscle is a small triangular muscle lying anterior to the rectus abdominis muscle that can be absent in approximately 20% of individuals. The pyramidalis muscle is contained in the rectus sheath and originates from the bony pelvis, where it is attached to the pubic symphysis and pubic crest through tendinous fibers. The fibers run superiorly and medially to insert into the linea alba, tensing it during muscle contractions.
Deep to the transversalis fascia and superficial to the parietal peritoneum lie structures which form several peritoneal folds divided by fossae. The median umbilical ligament, a remnant of the urachus, lies in the median line and makes the median umbilical fold of the parietal peritoneum. Lateral to it on both sides lay the supravesical fossae, laterally bounded by medial umbilical ligament pair which are remnants of the umbilical arteries. Each median umbilical ligament is covered through the medial umbilical fold. Medial inguinal fossae are located lateral to the medial umbilical folds. The lateral umbilical folds are made by the inferior epigastric vessels. Lateral to them lies the lateral inguinal fossae.
Nerves and vessels
Musculophrenic artery (Arteria musculophrenica);
Superficial epigastric artery (Arteria epigastrica superficialis);
the anterolateral abdominal wall is a large structure formed by multiple layers of skin, connective tissue, and muscles. These require an abundant blood supply, which is provided by different blood vessels. The arteries of the anterolateral abdominal wall can be divided into superficial layers and deep layers. The superficial branches include:
The musculophrenic artery is a branch of the internal thoracic artery. The musculophrenic artery supplies the superior part of the superficial anterolateral abdominal wall.
Superficial epigastric artery and lateral to it the superficial circumflex iliac artery. They are branches of the femoral artery and supply the inferior part of the abdominal wall.
The deepest layers of the anterolateral abdominal wall are supplied by the following:
The internal thoracic artery terminal branch is a superior epigastric artery. It runs in the rectus sheath behind the rectus muscle and supplies the superior part of the abdominal wall.
The inferior epigastric artery and deep circumflex iliac artery, both branches from the external iliac artery, supply the inferior part of the abdominal wall. The inferior epigastric artery enters the rectus sheath after piercing the fascia transversalis and it ends by anastomosing with the superior epigastric artery.
The 10 and 11 numbers intercostal arteries and subcostal arteries supply the lateral part of the abdominal wall.
There is a network of superficial veins that radiate out from the umbilicus and small paraumbilical veins which interconnect the network. The deep veins follow the same name arteries. The skin and peritoneum of the anterior and lateral abdominal wall are innervated by the T7 to L1 spinal nerves, which run in an inferior and medial direction. They give off lateral and anterior cutaneous branches along with their course. Muscles of the anterior abdominal wall are supplied by the lower 6 numbers thoracic nerves, the iliohypogastric nerve, and the ilioinguinal nerve.
Inguinal region
The anterior abdominal wall has naturally occurring paired canals in the lateral lower regions called inguinal canals. These oblique intramuscular tunnels can range from 3 to 5 cm long in an adult. They serve as a conduit that allows the passage of the male gonads from their intra-abdominal point of origin to their last destination in the scrotal sac. Each inguinal canal originates superolateral at the deep inguinal ring located at the medial half of the inguinal ligament of Poupart. The canal then terminates at the superficial inguinal ring, which is found approx 1 cm superolateral to the pubic tubercle.
In women, the round ligament of the uterus passes through each canal. Male inguinal canals convey the spermatic cord, which consists of the vas deferens, its related neuro vasculature, lymphatics, and connective tissue. Superficial and deep inguinal rings impose weak points in the abdominal wall and can create a predisposition to inguinal hernias.
Posterior Abdominal wall

Fascia
Thoracolumbar fascia (Fascia thoracolumbalis)
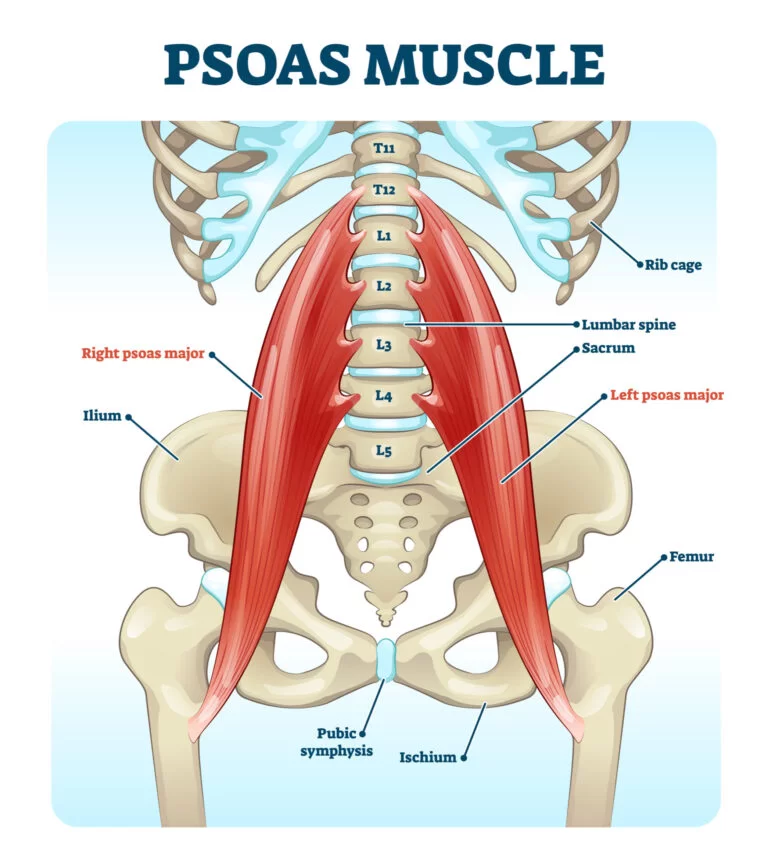
Analogously to the anterolateral abdominal wall, the fascia of the posterior abdominal wall lies immediately under the skin and subcutaneous tissue. The thoracolumbar fascia is a large, roughly diamond-shaped area of connective tissue that is formed by the thoracic and lumbar parts of the deep fascia. The thoracolumbar fascia is continuous with the transversalis fascia of the anterolateral abdominal wall and it is divided into three layers: anterior, middle, and posterior layers. The intrinsic deep back muscles are enclosed between the posterior layers and middle layers, while the quadratus lumborum muscles lay between the middle layers and anterior layers. More profound to the anterior layer runs the psoas major muscle with psoas fascia.

Posterior Abdominal wall Muscles
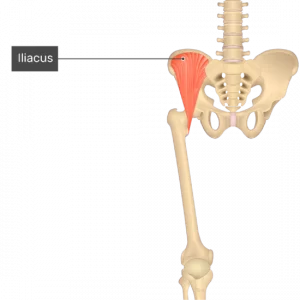
The posterior abdominal wall is supported by the 12th thoracic and all 5 lumbar vertebrae, along with their corresponding intervertebral discs. Three or four muscles are available in the posterior abdominal wall, depending on the individual: psoas major, iliacus, quadratus lumborum, and psoas minor muscles. The latter is variable, being present in about 40% of the total population. Note that the quadratus lumborum is the only ‘true’ posterior abdominal muscle, while the others muscles extend into the lower limb.
Psoas major muscle is a triangular, bilaterally paired muscle that forms part of the floor of the paravertebral gutter. It joins the iliacus muscle to form the iliopsoas muscle, the strongest hip flexor in the human body. The iliopsoas muscle is important for standing, walking, and running.
Quadratus lumborum muscle has medial attachments to the transverse/coastal processes of L1 to L4 and superior attachments to the inferior border of the 12th rib. The paired muscle acts by stabilizing the caudal connections of the diaphragm, while its unilateral contraction causes lateral flexion of the trunk. The bilateral contraction causes depression of the thoracic rib cage during inspiration and extends the trunk. Psoas minor muscle is a variable muscle present in only about 40% of the population. Its contraction leads to weak lateral flexion of the trunk.
Nerves and vessels
Subcostal artery (Arteria subcostalis)
Lumbar arteries (Arteriae lumbales)
Branches are derived from the descending aorta and supply the posterior abdominal wall. These include paired subcostal arteries, which run right under the 12th ribs, and four pairs of lumbar arteries arising from the back of the aorta. A variable 5th pair of lumbar arteries arising from the median sacral artery can be present. Subcostal and lumbar arteries anastomose with one another and with the superior epigastric, lower intercostal, and iliolumbar arteries supply the posterior abdominal wall and related structures. Venous drainage of the posterior abdominal wall is carried out mainly by the lumbar veins which empty into the inferior vena cava(IVC).
There is a plethora of nerves and vessels coursing through the abdominal cavity which are closely related to the posterior wall of the abdominal. It includes the abdominal aorta and its major branches, inferior vena cava with its tributaries, lumbar plexus, sympathetic ganglion chain, and sympathetic plexus. The lumbar plexus is formed by the divisions from L1 to L4 spinal nerves with the contribution of T12, which merge on the anterior surface of psoas major.
Clinical Importance of the Abdominal Wall:
Abdominal wall Provide a durable and flexible covering to prevent the abdominal viscera from leaving the abdominal cavity. Protecting internal abdominal organs from trauma or injury. Helps to maintain the anatomical position of the abdominal organs. Assist in expiration by pushing the abdominal organs towards the diaphragm.
Abdominal wall defect
Abdominal wall defects are a type of congenital defect that allows the stomach, the intestines, or other organs to protrude through the unusual opening which is forms on the abdomen.
During the development of the fetus, many unexpected changes occurred inside the womb. Specifically, the stomach, intestines, or other organs begin to develop outside the fetus’ abdomen through the abnormal hole in the abdomen and, as the progression of development, the abdominal wall eventually encloses these organs. In some cases of abdominal wall defect either the umbilical opening is too oversized or has developed improperly which allows the organs to remain outside or to squeeze through the abdominal wall.
There are two main types of abdominal wall defects that result due to changes while development. They are omphalocele and gastroschisis. Gastroschisis develops when the abdominal wall does not close completely, and the organs are present outside of the infant’s body. Omphalocele occurs when some of the organs protrude through the abdomen muscles in the area surrounding the umbilical cord. Omphalocele can be either minor, in which only some of the organs are exposed, or severe, with most, if not all of the abdominal organs being exposed.
Omphalocele
Omphalocele or exomphalos is a birth defect of the central portion of the anterior abdomen in which the herniated organs like the intestines and sometimes other abdominal organs such as the liver are covered by a thin membrane. At times, the membrane which consists of the peritoneum and amnion might be ruptured or matted. The key finding in omphalocele is that the herniation occurs centrally the organs herniate through an enlarged umbilical ring, with the umbilical cord inserted in the distal part of the membrane covering the defect.
Gastroschisis
Gastroschisis is a birth defect of the anterior abdominal wall accompanied by herniation of the small intestine and part of the large intestine, and sometimes other abdominal organs. Two key findings in gastroschisis are location, the defect is lateral to the inserted umbilical cord (commonly to the right), and covering there is an absence of a covering membrane, though the herniated organs might at times be covered by fibrous material due to in utero exposure to fluids.

2 Comments