
Elbow Joint: Anatomy, Bone, Muscles, Ligament, Importance
The elbow joint is the joint where the arm meets the body. It is made up of three bones: the humerus, or upper arm bone, and the radius and ulna, the bones of the lower arm.
The main purpose of the elbow joint is to allow the arm to move in a wide range of directions and to provide stability. It also allows us to bring our hands together and use them to interact with our environment.
Table of Contents
Introduction
~The elbow joint is a complex hinge joint formed between the distal end of the humerus in the upper arm and the proximal ends of the ulna and radius in the forearm.
~The elbow allows for the flexion and extension of the forearm relative to the upper arm, as well as rotation of the forearm and wrist.
Anatomy of Elbow joint
There are actually three joints at the elbow.
- Humeroulnar joint – Hinge joint formed between the humerus and the ulna. Allows flexion and extension of the elbow
- Humeroradial joint– Between the radius and humerus. Participates in flexion and extension but more importantly in supination and pronation of the forearm.
- Proximal radioulnar joint – A pivot joint formed by the radius and ulna. It participates in supination and pronation as well.
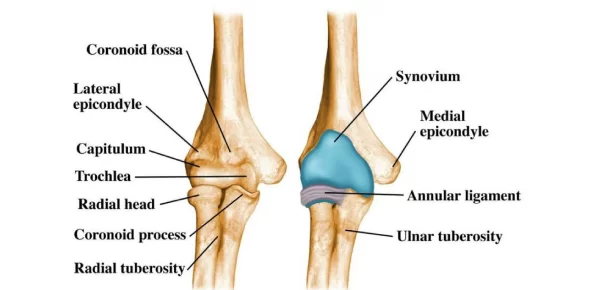
~The rounded distal end of the humerus is divided into two joint processes -— the trochlea on the medial side and the capitulum on the lateral side.
~The pulley-shaped trochlea forms a tight joint with the trochlear notch of the ulna surrounding it.
~On the lateral side, the concave end of the head of the radius meets the rounded, convex capitulum to complete the elbow joint.
~The loose union of the capitulum of the humerus and the head of the radius allows the radius to pivot as well as flex and extend. The pivoting of the radius allows for the supination and pronation of the hand at the wrist.
~Like all other synovial joints, a thin layer of smooth articular cartilage covers the ends of the bones that form the elbow joint. The joint capsule of the elbow surrounds the joint to provide strength and lubrication to the elbow.
~Slick synovial fluid produced by the synovial membrane of the joint capsule fills the hollow space between the bones and lubricates the joint to reduce friction and wear.
~An extensive network of ligaments surrounding the joint capsule helps the elbow joint maintain its stability and resist mechanical stresses. The radial and ulnar collateral ligaments connect and maintain the position of the radius and ulna relative to the epicondyles of the humerus.
~The annular ligament of the elbow extends from the ulna around the head of the radius to hold the bones of the lower arm together. These ligaments allow for movement and stretching of the elbow while resisting dislocation of the bones.
~Being a hinge joint, the only movements allowed by the elbow are flexion and extension of the joint and rotation of the radius. The range of motion of the elbow is limited by the olecranon of the ulna so the elbow can only extend to around 180 degrees. Flexion of the elbow is limited only by the compression of soft tissues surrounding the joint.
~Because so many muscles originate or are inserted near the elbow, it is a common site for injury. One common injury is lateral epicondylitis, also known as tennis elbow, which is an inflammation surrounding the lateral epicondyle of the humerus.
~Six muscles that control backward movement (extension) of the hand and fingers originate on the lateral epicondyle.
~Repeated strenuous striking while the muscles are contracted and against force — such as that occurring with the backhand stroke in tennis — causes strain on the tendinous muscle attachments and can produce pain around the epicondyle. Rest for these muscles will usually bring about recovery.
Joints:
Radioulnar joint:
~trochoid or pivot type of joint.
~radial head rotates around at proximal ulna.
~distal head rotates around at distal ulna.
~annular ligament maintains radial head into its joint.
*supinate 80-90 degrees from neutral.
*pronate 70-90 degrees from neutral.
*joints between shaft between radius and ulna head tightly together between proximal and distal articulations by an interosseous membrane.
*Articulating Surfaces:
~It consists of two separate articulations:-
- The trochlear notch of the ulna and the trochlea of the humerus
- Head of the radius and the capitulum of the humerus
In the anatomic position [elbow is extended, the forearm is supinated], the long axis of the forearm has a lateral inclination or valgus at the elbow. This is called the carrying angle and is measured to be 13± 5 degrees for females and 11 ± 4 for females.
Bones of Elbow Joint
~The elbow joint is composed of the distal end of the humerus and the proximal ends of the radius and the ulna.
Distal End of Humerus:
~Humeral condyle, the distal end of the humerus is made up of the capitellum laterally and the trochlea medially. This condyle is covered by articular cartilage and articulates with the trochlear notch of the ulna and the concave superior aspect of the head of the radius.
~The axis of the trochlea is externally rotated by 3 -8 degrees and compared with the longitudinal axis is in 4- 8° of valgus. The articular surface of the trochlea and capitellum is projected anteriorly at an angle of 40° to the axis of the humerus.
~The trochlea, the distal medial articulating end of the humerus acts as a pulley for the ulnar trochlear notch to rotate around as the elbow is flexed.
~The capitellum is a rounded ball of bone that adjoins the trochlea laterally. It is the distal lateral articulating end of the humerus. It articulates with the radial head.
~Superior to the articulating surface, the middle of the width of the humerus is marked by two depressions. On the anterior surface, it is the coronoid fossa that accommodates the coronoid process of the ulna on flexion. Lateral to it is a smaller fossa called radial fossa that accepts radial head on flexion.
~A depression on the posterior aspect is called the olecranon fossa which accommodates the olecranon of the ulna on the extension. The olecranon is the proximal end of the ulna, from which the C-shaped trochlea notch is carved.
~Lateral to the humeral condyle are the medial and lateral epicondyles, and superior to those on their respective sides are the medial and lateral supracondylar ridges.
~The epicondyles and ridges serve as attachment sites for ligaments and muscles. The medial epicondyle serves as the origin of flexor muscles of the forearm and hand whereas lateral epicondyle serves as the extensor origin.
Ulna:
~The upper end of the ulna provides an articular cartilage–a covered trochlear notch carved out of the olecranon process. The olecranon posteriorly serves as an attachment of the triceps muscle, a powerful elbow extensor.
~Anteriorly, the trochlear notch ends in a blunt central point called the coronoid process.
~The tuberosity of the ulna lies inferior to the coronoid process on the anterior aspect of the ulna. After that, further distally, is the shaft.
~Laterally the coronoid process is the radial notch, in which lies the head of the radius.
Radius:
~Head of the radius bone is the main participant in the elbow joint. Its superior aspect contributes to the hinge portion of the elbow joint. The medial circumferential aspect of the head of the radius forms the radioulnar articulation.
~After the head, the bone narrows distally into the neck. Anteromedially, a thick structure is called Distal to the head of the radius is a narrowing of the bone, referred to as the neck, and anteromedially is the radial tuberosity, followed distally by the shaft.
Key bony landmarks:
~medial epicondyle
~lateral epicondyle
~lateral supracondylar ridge
Bony landmarks:
~medial condiloid ridge
~olecranon process
~coronoid process
~radial tuberosity
Elbow movement:
~primarily involves movement between articular surfaces of the humerus and ulna.
~specifically humeral trochlear fitting into the ulnar trochlear notch.
~radial head relatively small amount of contact with the capitulum of the humerus.
~as the elbow reaches full extension, the olecranon process is received by the olecranon fossa.
*increased joint stability when fully extended.
~as the elbow flexes 20 degrees or more, its bony stability is unlocked, allowing for more side-to-side laxity.
~stability in flexion is more dependent on the lateral (radial collateral ligament) the medial or (ulnar collateral ligament)
Joint Capsule and Ligaments of the Elbow joint:
~The joint capsule is contiguous between the hinge and radioulnar aspects of the joint. The capsule has an outer fibrous layer and an inner synovial layer.
~The superior aspect of the joint capsule begins just superior to the coronoid and olecranon fossae and continues inferiorly, covering just past the proximal radial-ulnar articulation.
~The ulnar collateral ligament is a medial thickened part of the capsule.
~Ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid and olecranon of the ulna. It is a triangular thickening with 3 main bands
- Anterior or cord-like band
- A posterior fan-like band
- Oblique band
- The oblique band also helps to deepen the trochlear notch.
~The radial collateral ligament is the lateral thickening and extends from the lateral humeral epicondyle and distally blends into the annular ligament of the radius.
~The annular ligament of the radius wraps around the head of the radius and attaches to the ulna anteriorly and posteriorly. It allows the head of the radius to rotate inward during supination and pronation while maintaining the stability of the radial ulnar joint.
Bursae of Elbow Joint:
- Intratendinous – located within the tendon of the triceps brachii.
- Subtendinous – between the olecranon and the tendon of the triceps brachii.
- Subcutaneous – between the olecranon and the overlying connective tissue.
Blood Supply
The blood supply to the elbow joint is by the branches from the periarticular arterial anastomoses of the elbow.
~the inferiorlateral cutaneous nerve of the arm and the posterior cutaneous nerve of the forearm supply lateral elbow. The medial cutaneous nerve of the forearm supplies sensation to the medial aspect of the elbow. The cubital fossa is supplied by the musculocutaneous nerve (the lateral cutaneous nerve of the forearm).
~The skin over the joint belongs anteriorlaterally to C6 dermatome and anteromedially to C5, C8, and T1 dermatomes. Posteriorly, the C6 dermatome laterally and the C8 dermatome medially are split down the middle by the C7 dermatome.
Nerve Supply:
- Ulnar nerve
2. Median nerve
3. Radial nerve
4. Musculotaneous nerve through its branch to the brachialis.
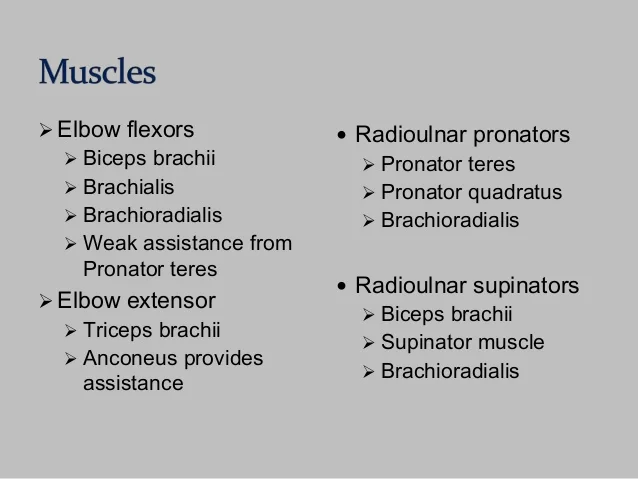
Muscles of the Elbow Joint:
Clinical Importance of Elbow Joint:
~ The elbow joint is a frequently injured joint and the site for many disorders.
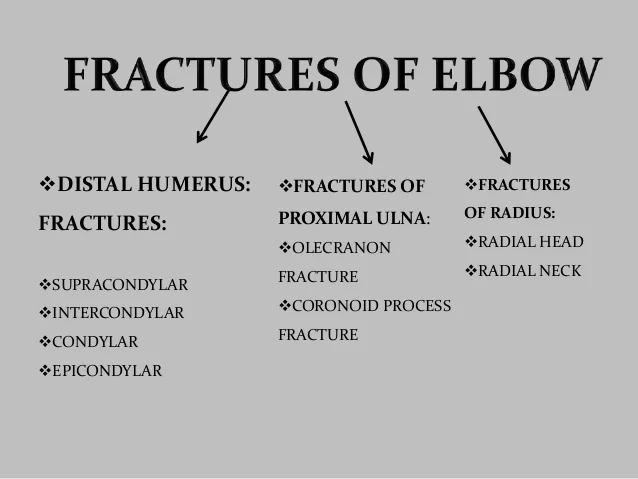

Supracondylar fracture:
~this is the most common fracture occur around the elbow in children.(60%)
~usually the distal fracture fragment diplaces posteriorly.
~The fracture line extends transversly or obliquely through the distal humerus above the condyles.
Intercondylar fracture:
~the fracture line extends between the medial and lateral condyles and communicates with the supracondylar region.
~the resultant fracture may take on a T OR Y configuration.
~ this type of fracture in adults accounts for at least 50% of distal humeral fractures.
~the transverse fracture line that passes through both humeral condyles is called a transcondylar fracture.
~ a comminuted fracture of the distal humerus, usually with associated ulnar and radial fractures, may occur if an object is struck with the elbow protruding from a car window.
Epicondylar Fracture:
~ separation of the medial epicondyle is a common injury in sports in which strong throwing actions are performed, such as baseball.
~epicondylar fractures are usually avulsive injuries from the traction of the respective common flexor or extensor tendons and the collateral ligament on the medial or lateral epicondyle.
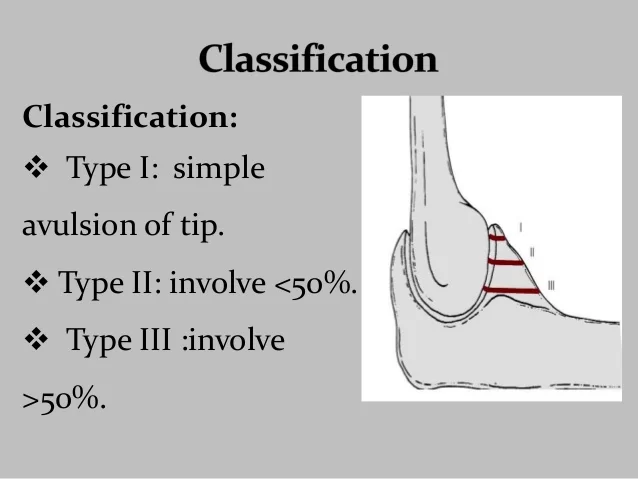
*Classification:
*type-1:-large fragment of the bone and articular surfces(Involves trochlea) are fractured.
*type-2:-small shell of bone and articular surface 9not involves trochlea).
*type-3:-comminuted fracture
*Fractures of the Proximal Ulna:
*Olecranon fracture:
*mechanism of injury:
~ direct fall on the flexed elbow, and this frequently produces comminution and marked displacement of the major fragments.
~indirect:-fall on the outstretched arm, produces an oblique or transverse fracture with minimal displacement.
~imaging:-well demonstrated on a lateral projection of the elbow.
*Avulsion fracture:
*Coronoid fracture:
~it indicates severe trauma to the elbow.
~mechanism of injury:-
~striking of trochlea in coronoid.
~(avulsion) less common.
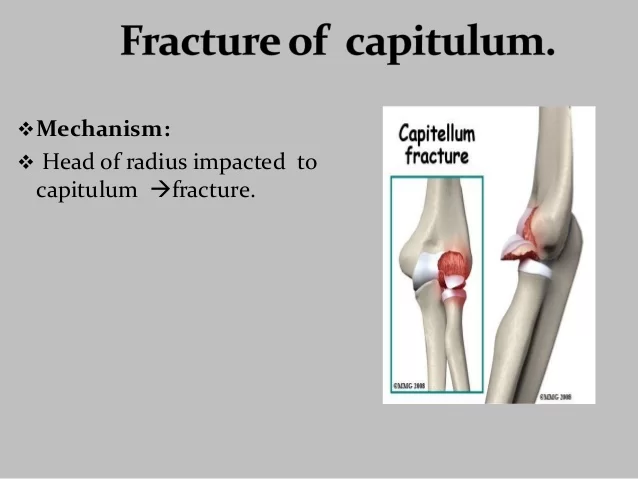
*Fracture of the radial head:
~it is common in adults.
~mechanism of injury:-
~ F.O.R.H. While the arm is pronated, the head is impacted in the capitulum.
*classification:
~type-1:-undisplaced
~type-2:-displaced
~type-3:-comminuted
~type-4:-associated with posterior elbow dislocation and coronoid fracture.
*Radial neck fracture:
~the most common radial neck fracture is an impaction at the junction of the head and neck.
~the only sign may be a sharpened angle on the anterior surface, best depicted on the lateral projection.
~complete fractures will be readily seen as a transverse lucent line with varying degrees of displacement.

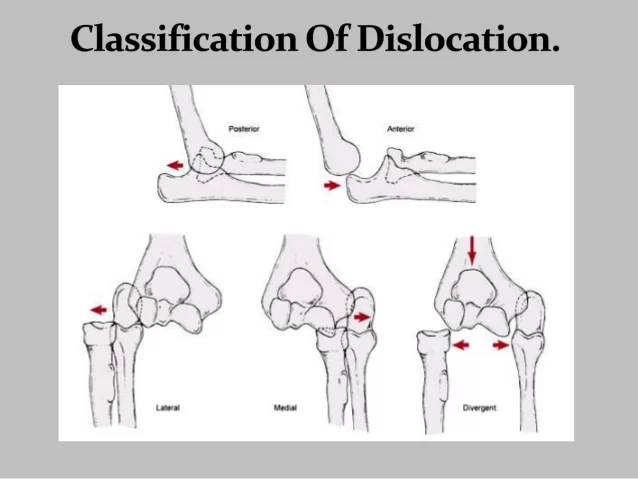
*Dislocation of Elbow:

~Dislocation of the elbow could occur in isolation or as part of more severe trauma which may cause fracture of the bones too.
Pulled Elbow:
~In children, when a distraction force is applied along the long axis of the forearm from a point distal to the elbow, the head of the radius can be pulled out of the annular ligament that holds it in place. This injury is called “pulled elbow” and occurs in young children. The injury usually involves a parent or other adult figure lifting a child up vertically with a single hand.
Lateral epicondylitis:
~Lateral epicondylitis is also called tennis elbow and involves inflammation of the common extensor origin at the lateral epicondyle of the humerus. Repetitive extension movements at the wrist cause pain.
Medial epicondylitis:
~Medial epicondylitis or golfer’s elbow is an inflammation of the common flexor origin at the medial epicondyle of the humerus. Repetitive flexion movements at the wrist cause an overuse of pain at the site.
Cubital tunnel syndrome:
~Cubital tunnel syndrome is caused by compression of the nerve as it passes in a groove behind the medial epicondyle of the humerus or cubital tunnel. Paresthesias in the distribution of the ulnar nerve is the chief complaint.
Pronator syndrome:
~Compression neuropathy of the median nerve as it passes between the two heads of the pronator teres muscle. The syndrome can cause paresthesias in the distribution of the median nerve distal to the compression and may lead to weakness in the flexor pollicis longus, the flexor digitorum profundus laterally, and the pronator quadratus.
Olecranon bursitis:
~Olecranon bursitis or student’s elbow is an inflammation of the olecranon bursa at the proximal aspect of the posterior ulna. It can be caused by trauma, infection, prolonged pressure, or other conditions. The bursa is swollen and is often painful.
FAQs
The elbow joint is a hinge joint that offers excellent mobility and stability for carrying out regular tasks. We are able to do daily tasks because of the powerful muscles that span the elbow joint, which causes flexion, extension, supination, and pronation.
Arthritis of the elbow
There are several kinds of arthritis that can affect the elbow. The most prevalent kind of arthritis is osteoarthritis. The thin layer of cartilage that surrounds the bones of a joint provides protection, and this is where it all begins.
The elbow joint’s role is to flex and extend the arm’s grip and reach for items. The elbow has a range of motion that extends from 0 degrees to 150 degrees of flexion.
Located between the arm and the forearm in the upper limb lies the elbow joint, a synovial joint. There are three bones that articulate at this point: the forearm’s ulna, radius, and humerus. In terms of structure, the elbow joint is categorized as a synovial joint.
Five muscles that are related to the elbow joint are innervated by the radial nerve:
the triceps brachii
the anconeus
the brachioradialis
the supinator muscle
the brachialis
Radius
The forearm’s smaller bone, the radius, is located on the joint’s outside. Because the radius head is hollow and round, it can move with the humerus. The ulna-radius link facilitates the rotation of the forearm.


11 Comments