Forequarter Amputation: Treatment, Prosthesis, Complication
Table of Contents
Definition Of Forequarter Amputation
Forequarter Amputation is carried out proximal to the shoulder joint. It is indicated for malignant tumors of bone in the upper end of the humerus. In this, part of the scapula and clavicle are removed along with the shoulder girdle muscles.

Indication of Forequarter Amputation:
The most common indications for forequarter amputation are unresectable bone and soft-tissue sarcomas, axillary sarcomas that involve the brachial plexus and axillary artery, recurrent sarcomas following radiation therapy, or those bony tumors that progress on induction chemotherapy.
Multidisciplinary team:
- diabetologist
- podiatrist
- microbiologist
- nurse
- orthopedic surgeon
- vascular surgeon
- Psychologist
- Physiotherapist
What are the responsibilities of the team?
- Evaluate the patient
- Ensure medical stability of the patient
- Prepare the patient’s life as an amputee
- Prescribe prosthesis (if appropriate)
- Fabricate prosthesis
- Evaluate fit of the prosthesis Educate the patient about the use and care of the prosthesis
- Follow-Up care for the patients
Treatment:
Surgical Treatment:
OPERATIVE TECHNIQUE FOREQUARTER AMPUTATION :
- The surgical technique for the present case of forequarter amputation was described by Berger in 1887.
- The patient was placed in a right lateral decubitus position to expose the thorax, with the left upper limb freely able to rotate.
- An anterior approach was used for forequarter amputation.
- A modified elliptical incision was made with the superior apex over the clavicle on one end and it is continued inferior and laterally.
- The inferior apex was made at the midaxillary line and it is continued posterosuperior over the entire length of the scapula to join the superior apical incision.
- Soft-tissue dissection was at the fascial level over the pectoralis major muscles.
- The clavicle was exposed and divided at the proximal third; care was taken not to tear the underlying vein.
- The clavicle bone was carefully elevated to expose the subclavian artery, vein, and brachial plexus.
- The subclavian artery was ligated and cut first, then the subclavian vein was tied and cut to stop bleeding from the collateral blood supply of the shoulder.
- Brachial plexus Branches were ligated and divided proximally. Next, the chest wall attachments of the pectoralis major and minor muscles were divided.
- Posteriorly, fasciocutaneous skin flaps were developed and all of the periscapular muscles were released. This causes the shoulder girdle to be freed and the whole extremity to fall away from the trunk.
- The anterior and posterior flap of the skin was used to close the defect primarily.
- Any excess dog-ear skin was excised and closed primarily, and drainage was placed.
Physiotherapy treatment for Forequarter amputation:
- Psychological counseling to the patient
- Psychological support
- Providing information is important
- to decrease the anxiety of patients and their family members.
- obtain cooperation in the treatment program
- to help the patient with an amputation to adjust to his new condition.
- A feeling of a complete change in reality due to lack of functional activity.
Breathing exercise :
to prevent the accumulation of fluid
to prevent chances of infections
Postural advice during sitting, standing, and walking
Active ROM
- Cervical spine:
- Flexion
- Extention
- Right side rotation
- Left side rotation
- Right side flexion
- Left side flexion
Active exercise of normal upper limb extremities :
- Glenohumeral joint :
- Flexion
- Extention
- Abduction
- Adduction
- Internal Rotation
- External Rotation
- Scapula:
- elevation
- depression
- protraction
- retraction
- Elbow :
- flexion
- Extention
- Forearm:
- Supination
- pronation
Strengthening Exercise:
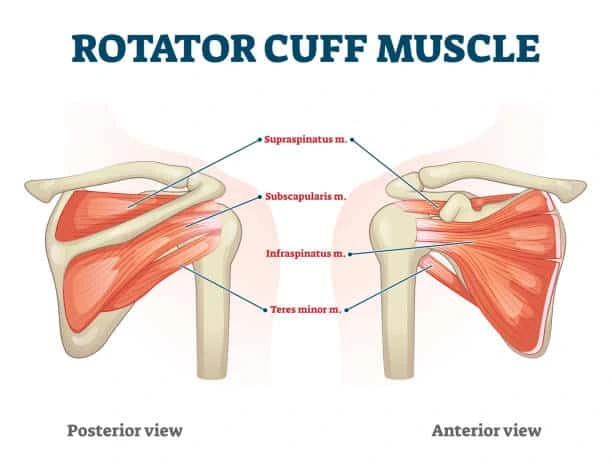
Strengthening Exercise of Neck Flexors, Extensors, Rotators, side flexors, and Scapular muscles (rotator cuff muscles, teres major, subscapularis, teres minor, and infraspinatus)
Strengthening exercise of the pectoralis major and pectoralis minor
The physiotherapist will:
Teach donning (putting on) and doffing (taking off) of the prosthesis.
Build up muscle strength and power.
Teach coordination skills that will assist with activities of daily living(ADL) such as dressing and washing etc.
Try to address any obstacles that may prevent a return to work and previous hobbies of patients.
Prosthesis for Forequarter Amputation :
The whole upper extremity is removed along with the scapula and clavicle. A plastazote cap, padded with foam and retaining straps, can be given. Only a sleeve fitter cosmetic prosthesis may be given.

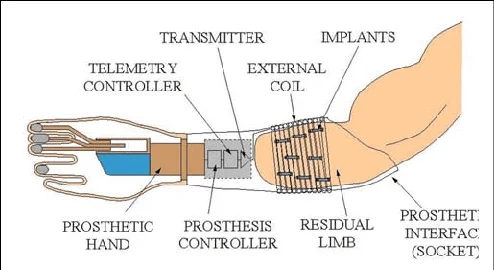
Myoelectric Prosthesis :
The complication of Forequarter amputation :
- Excess bleeding
- Blood clots
- Edema
- Poor healing
- deep vein thrombosis (DVT)
- wound infection
- pneumonia
- “phantom limb” pain
- depression
- Stump ulceration
- Flap necrosis
- Joint stiffness
- Osteomyelitis
- Osteoporosis