

Muscles Of Back: Anatomy, Origin, Insertion, Function
The muscles of the Back are divided into three-layer – The superficial layer, the intermediate layer, and the Deepest layer the muscles.
Superficial muscles of the back :
The superficial back muscles are the muscles found just below the skin. Within this group of back muscles, you will find the latissimus dorsi, the trapezius, levator scapulae, and the rhomboids.
Intermediate muscles of the back :
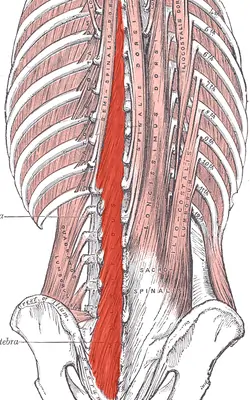
The intermediate muscles are the erector Spinae. They contain the longissimus, iliocostalis, and Spinalis muscles. Their attachments subdivide these muscles, and they all have a commonest tendinous origin. They play an important role in the movement of the thoracic cage and flexion of the upper vertebral column and head.
Deep muscles of the back :
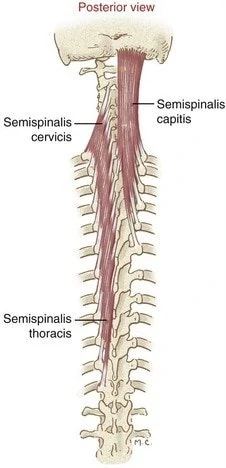
The deep muscles of the back include the semispinalis, multifidus, and rotatores. These muscles help to stabilize the vertebral column and also have a role in proprioception and balance. Moreover, these muscles help with the movements of the vertebral column and also help to maintain posture.
Superficial layer: splenius (splenius Capitis, splenius Cervices, latissimus dorsi, trapezius, levator scapulae, and the rhomboid minor and rhomboid major)
Intermediate layer: erector spinae (iliocostalis, longissimus, spinalis)
Deep layer: transversospinales (semispinalis, multifidus, rotatores)
The deepest layer of Muscles: segmental muscles (Levatores Costarum, Interspinales, and Intertransversarii)
Table of Contents
Superficial muscles of the Back:
Superficial muscles of the back includes :
Splenius Capitis Muscle (Musculus splenius Capitis);
Splenius cervices muscle (Musculus splenius Cervices);
The splenius Capitis

Origine :
the spinous processes of vertebrae C7 to T3 and the lower half of the nuchal ligament.
Insertion :
inserted over the mastoid process and the lateral third of the superior nuchal line of the occipital bone.
blood supply :
blood supplies are the vertebral, occipital, superior intercostal, deep cervical, and transverse cervical arteries.
Nerve supply :
innervation of splenius Capitis are posterior rami of the middle cervical spinal nerves and lower cervical spinal nerves
Action :
lateral flexion of the neck and rotation of the neck to the same side.
The Splenius Cervices
Origine :
the spinous processes of vertebrae T3-T6
Insertion :
the transverse processes of vertebrae C1 to C3 or C4.
blood supply :
the blood supply of splenius Cervicis vertebral, occipital, superior intercostal, deep cervical, and transverse cervical arteries.
Nerve supply :
splenius Cervicis innervated by posterior rami of the middle cervical spinal nerves and lower cervical spinal nerves
Action :
lateral flexion of the neck and rotation of the neck to the same side.
Latissimus dorsi
Origin :
spinous processes of thoracic T7 to T12, thoracolumbar fascia, iliac crest, and inferior 3 or 4 ribs, inferior angle of the scapula
Insertion :
As the latissimus dorsi inserts into the floor of the intertubercular groove of the humerus, it is surrounded by two major muscles. The teres major inserts medially on the medial lip of the intertubercular groove and the pectoralis major inserts laterally onto the lateral lip of the intertubercular groove.
Nerve supply :
The thoracodorsal nerve, a branch of the posterior cord of the brachial plexus (C6 to C8 with C7 predominant) provides innervation to the latissimus dorsi muscles.
Blood supply :
the latissimus dorsi muscles receive blood supply from dorsal perforating branches of the lower three posterior intercostal arteries and the upper three lumbar arteries.
Action :
adduction, medially rotation, and extension of the upper limb at the glenohumeral joint.
Trapezius
Origin :
The muscle attaches to the medial third of the superior nuchal line; external occipital protuberance, nuchal ligament, and spinous processes of C7 to T12 vertebrae.
Insertion :
Trapezius muscle inserts on the lateral third of the clavicle, acromion, and spine of the scapula.
Nerve Supply :
The spinal root of the accessory nerve (CN XI) (motor)
C3 and C4 Cervical nerves (pain and proprioception)
Blood Supply :
Transverse cervical artery (cervicodorsal trunk)
Action :
The function of the trapezius muscles is to stabilize and move the scapula. The upper fibers of the trapezius elevate and upwardly rotate the scapula and extend the neck. The middle fibers of the trapezius adduct (retract) the scapula. The lower fibers of the trapezius depress and aid the upper fibers in upwardly rotating the scapula.
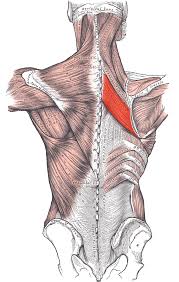
Levator scapulae
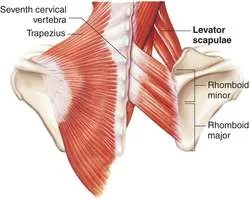
Origin :
The levator scapulae originate from the posterior tubercle of the transverse process of cervical vertebrae C1 – C4.
Insertion :
The muscle is inserted into the medial border of the scapula extending from the superior angle to the junction of the spine and medial border of the scapula.
Nerve Supply :
cervical nerve (C3 and C4) and dorsal scapular nerve (C5).
Blood Supply :
dorsal scapular artery
Action :
The action of the Levator scapulae is to an elevation the scapula and tilt the glenoid cavity inferiorly by rotating the scapula downward.
Rhomboid minor:
Origin :
The rhomboid minor is a cylindrical muscle that originates from the Ligamentum nuchae and C7 and T1 vertebrae.
Insertion :
Rhomboid minor inserts at the scapula’s medial border near the base of the spine of the scapula. The rhomboid major is a quadrangular muscle located inferior to the rhomboid minor muscles.
Nerve Supply :
Rhomboid minor is supplied by the dorsal scapular nerve from the C5 root of the brachial plexus. Blood Supply :
dorsal scapular artery.
Action :
Retraction and rotation of the scapula fix the scapula to the thoracic wall
Rhomboid major:
Origin :
The origin of the rhomboid muscles is from the spinous processes of the T2 to T5 vertebrae
Insertion :
The rhomboid major is inserted on the medial border of the scapula, just inferior to the rhomboid minor.
Nerve Supply :
Rhomboid major is supplied by the ventral primary ramus via the dorsal scapular nerve (C5).
Blood Supply :
Dorsal scapular artery and deep branch of the transverse cervical artery.
Action :
retraction, elevation, and rotation of the scapula. The rhomboid major also protracts the medial border of the scapula, keeping it in position at the posterior thoracic wall.
Intermediate Back Muscles
This layer contains the large erector Spinae muscles, which are sometimes called the long muscles of the back. This muscle group is the largest of the deep muscles of the back and lies on either side of the vertebral column between the spinous processes of the vertebrae and the angles of the ribs.
The Intermediate layer muscles contain three vertical columns of muscle that lie side to side. From the lateral to the medial side, these are the iliocostalis, longissimus, and Spinalis muscles. Each column of muscle is subdivided into different regions (like Lumborum, thoracic, Cervicis, Capitis) based on which region of the axial skeleton it attaches to superiorly
Erector Spinae muscles
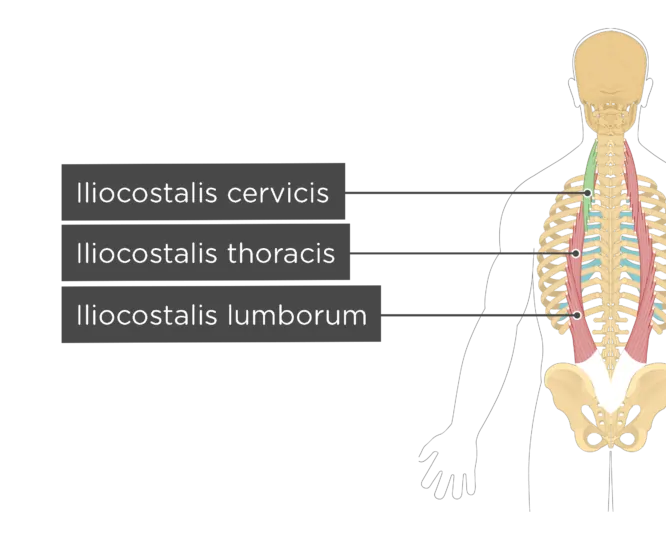
Iliocostalis
Iliocostalis muscle (Musculus iliocostalis);
The lateral column of the Erector Spinae muscle group is formed by the iliocostalis muscle.
The muscle is divided into three different regions according to its attachments:
Iliocostalis cervicis
Iliocostalis thoracic
Iliocostalis lumborum
Attachments of the iliocostalis muscle
Iliocostalis cervicis
Origin:
The angle of ribs 3-6
Insertion:
Transverse processes of vertebrae C4-C6
Blood supply :
The iliocostalis Cervicis is supplied by the occipital, deep cervical, and vertebral arteries.
Nerve supply :
The Nerve supply of the iliocostalis Cervicis is the lateral branches of the posterior rami of cervical, thoracic, and lumbar spinal nerves.
Action:
Laterally flexion and Extension of the lower cervical region
Iliocostalis Thoracis
Origin:
The angle of ribs 7-12
Insertion:
Angles of ribs 1 to 6, Transverse process of the C7 vertebra
Blood supply :
The iliocostalis Thoracis muscles are supplied by the dorsal branches of the posterior intercostal and subcostal arteries
Nerve supply :
The iliocostalis Thoracis muscles are innervated by lateral branches of the posterior rami of cervical, thoracic, and lumbar spinal nerves.
Action:
extension and lateral flexion of the Thoracic spine.
Iliocostalis lumborum
Origin:
Origin of Iliocostalis Lumborum is the Lateral crest of the sacrum, the medial end of the iliac crest, and the Thoracolumbar fascia
Insertion:
The angle of ribs 5 to 12, Transverse processes of vertebrae L1 to L4
Blood supply :
The iliocostalis Lumborum muscles are supplied by the dorsal branches of the lumbar and lateral sacral arteries.
Nerve supply :
The Nerve supply of the iliocostalis Lumborum muscles is the lateral branches of the posterior rami of cervical, thoracic, and lumbar spinal nerves.
Action :
Extension of the Spine: Acting bilaterally, extension and hyperextension of the spine.
Laterally flexion of the spine when acting unilaterally
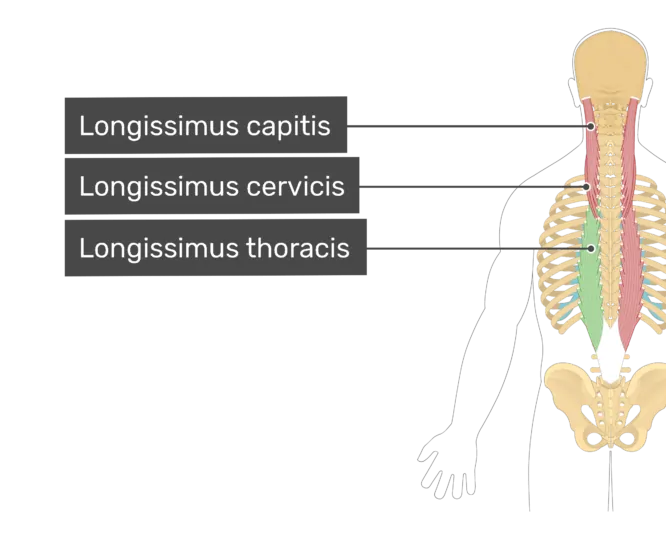
Longissimus
Longissimus muscle (Musculus longissimus);
The longissimus muscle forms the central column of the Erector Spinae muscle group and is the longest and thickest muscle in this group. It is divided into three regions according to their attachments:
Longissimus Capitis
Longissimus Cervicis
Longissimus Thoracis
Longissimus thoracis is further subdivided into thoracic and lumbar parts.
Attachments of the longissimus muscle
Longissimus Capitis
Origin:
Transverse processes of vertebrae C4 to T5
Insertion:
Mastoid process of the temporal bone
Nerve supply
Longissimus Capitis is innervated by the lateral branches of posterior/dorsal rami of cervical spinal nerves.
Blood supply :
Longissimus Capitis receive blood supply from the vertebral artery, deep cervical artery, superficial and deep descending branches of the occipital artery, and deep branch of the transverse cervical artery.
Longissimus Cervicis
Origin: Transverse processes of vertebrae T1-T5
Insertion: Transverse processes of vertebrae C2-C6
Nerve supply :
Longissimus Cervicis is innervated by the lateral branches of posterior/dorsal rami of cervical spinal nerves.
Blood supply :
Longissimus Cervicis receive blood supply from the vertebral artery, deep cervical artery, superficial and deep descending branches of the occipital artery, and deep branch of the transverse cervical artery.
Action :
Extension of the neck vertebrae. laterally flexion of the neck vertebrae to the same side.
Longissimus Thoracis
Lumbar part
Origin:
The origin of the Lumbar part of Longissimus thoracic muscles is Lumbar intermuscular aponeurosis, the medial part of the Sacropelvic surface of the ilium, posterior sacroiliac ligament
Insertion:
Accessory and transverse processes of vertebrae L1 to L5
Nerve supply :
the longissimus thoracis muscles are innervated by the lateral and intermediate branches of the posterior rami of the lumbar spinal nerves.
Blood Supply :
the posterior branches of superior intercostal, posterior intercostal, lateral sacral, and median sacral arteries.
Action :
spine extension and lateral flexion.
Thoracic part
Origin:
Spinous and transverse processes of vertebrae L1 to L5, median sacral crest, posterior surface of the sacrum, and posterior iliac crest
Insertion:
Transverse process of vertebrae T1 to T12, Angles of ribs 7 to 12
Nerve supply :
the medial and lateral branches of the posterior rami of thoracic spinal nerves.
Blood Supply :
the dorsal branches of superior intercostal, posterior intercostal, lateral sacral, and median sacral arteries.
Action :
spine extension and lateral flexion.
Spinalis
Spinalis muscle (Musculus spinalis);
Synonyms: Musculi Spinalis
The Spinalis muscle is the small and most medial of the Erector Spinae group of muscles.
Like the longissimus, the Spinalis muscle is also divided into three parts:
Spinalis Capitis
Spinalis Cervicis
Spinalis Thoracis
Attachments of the Spinalis muscle
Spinalis Capitis
Origin:
Spinous processes of vertebrae C7-T1
Insertion:
Occipital bone (midline)
Nerve supply :
The innervation of the Spinalis Capitis muscle comes from the lateral branches of the posterior/dorsal rami of adjacent spinal nerves (cervical, thoracic and lumbar).
Blood supply :
muscular branches of the vertebral, deep cervical, and occipital arteries supply Spinalis Capitis.
Action :
produced cervical extension as well as lateral flexion and rotation of the spine and head.
Spinalis Cervicis
Origin:
Spinous processes of vertebrae C7 to T1, nuchal ligament
Insertion:
The spinous process of vertebrae C2 to C4
Nerve supply :
The innervation of the Spinalis Cervicis muscle comes from the lateral branches of the posterior/dorsal rami of adjacent spinal nerves (cervical, thoracic and lumbar).
Blood supply :
muscular branches of the vertebral, deep cervical, and occipital arteries supply Spinalis Cervicis.
Action :
produced extension, lateral flexion, and rotation at the cervical spine level.
Spinalis Thoracis
Origin:
The spinous process of vertebrae T11 to L2
Insertion:
The spinous process of vertebrae T2 to T8
Nerve supply :
The innervation of the Spinalis Thoracis muscle comes from the lateral branches of the posterior/dorsal rami of adjacent spinal nerves (cervical, thoracic and lumbar).
Blood supply :
The Spinalis Thoracis muscle arterial is supplied by dorsal branches of the superior and posterior intercostal arteries, and branches of the lumbar arteries.
Action :
produced thoracic extension as well as lateral flexion and rotation of the spine.
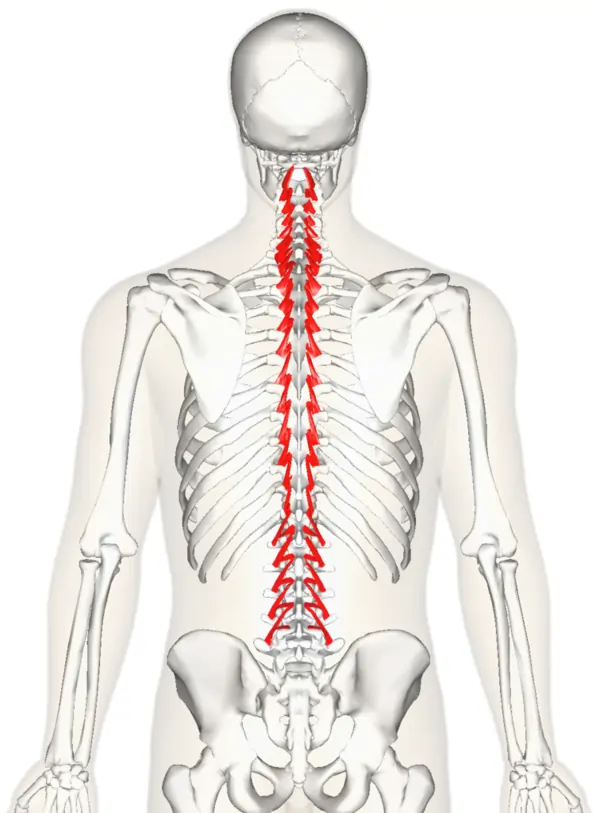
Multifidus
Multifidus muscle (Musculus multifidus);
This belongs to the intermediate layer of the transversospinalis muscles group. The multifidus muscle is composed of many short, triangular muscles that span the entire length of the vertebral column but are the thickest and most developed in the lumbar region. The multifidus is divided regionally into three parts:
Multifidus Cervicis
Multifidus Thoracis
Multifidus Lumborum
Multifidus Cervicis
Origin :
that arises from the superior articular processes of vertebrae C4 to C7.
Insertion :
lateral aspect and the tips of the spinous processes of C2 to C5 vertebrae.
Multifidus thoracic
Origin :
that originates from the transverse process of the thoracic vertebra.
Insertion :
lateral aspect and tips of the spinous processes of vertebrae 2 to 5 levels above the origin.
Multifidus Lumborum
Origin :
that arises from the mammillary processes of lumbar vertebrae, posterior aspect of sacrum, posterior superior iliac spine (PSIS) of the ilium, and posterior sacroiliac ligament.
Insertion :
lateral aspect and tips of the spinous processes of vertebrae 2 to 5 levels above the origin.
Nerve supply :
The nerve supply of the multifidus muscle is derived from the medial branches of the posterior rami of spinal nerves in the corresponding cervical, thoracic and lumbar regions.
Blood Supply :
multifidus muscle’s arterial supply comes from the vertebral, deep cervical, occipital, posterior intercostal, subcostal, lumbar, and lateral sacral arteries according to the regions the muscle parts occupy.
Function :
The multifidus muscle’s main function is to stabilize the vertebrae during movements of the spine. Bilateral contraction of the muscle results in extension of the vertebral column at all levels (cervical, thoracic and lumbar regions), while unilateral contraction produces ipsilateral( same side) lateral flexion and contralateral rotation of the vertebral column.
Rotatores
Rotatores breves and Rotatores Longi muscles (Musculi rotatores breves et Longi);
Synonyms: Thoracic rotatores muscles, Long rotatores muscles, and short rotatores muscles
Deep to the multifidus is the small rotator muscles, which are the deepest of this muscle group. The rotatores muscles are also present along the entire length of the vertebral column, but are more prominent and best developed in the thoracic area. They consist of short rotatores (rotatores breves) which attach to the spinous processes of adjacent superior vertebrae and long rotatores (rotatores Longi) which attach to two levels up vertebrae.
Attachments of the rotatores muscles
Rotatores breves
Origin:
Transverse processes of T2 to T12 vertebrae
Insertion:
Laminae/Spinous process of the vertebra (1 level above the origin)
Rotatores Longi
Origin:
Transverse processes of the thoracic vertebrae
Insertion:
Laminae/Spinous process of the vertebra (2 levels above the origin)
Nerve supply :
The rotatores are innervated by the medial branches of the posterior rami of spinal nerves.
Blood supply :
blood supply through dorsal branches of posterior intercostal and lumbar arteries.
Function :
the major function of the rotator muscles is to stabilize the spine. Bilateral contraction of these muscles causes extension of the vertebral column, while unilateral contraction causes rotation of the trunk of the contralateral side.
Deep muscles of the back
The Levatores Costarum, interspinal, and Intertransversarii muscles make up the deepest layer of the deep back muscles and are sometimes referred to as the segmental muscles or the minor deep muscles of the back.
Levatores Costarum
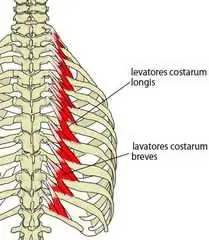
Levatores Costarum muscles (Musculi Levatores Costarum)
Synonyms: Levator Costae muscles
The Levatores Costarum muscles are located in the thoracic part of the vertebral column. They originate from the transverse processes of C7 to T11 vertebrae and travel inferolateral to insert between the tubercle and the angle of the corresponding rib below.
Nerve supply :
The Levatores Costarum are innervated by the lateral branches of the posterior rami of thoracic spinal nerves (T1 to T12).
Blood supply :
Levatores Costarum vascularized by the dorsal branch of the posterior intercostal artery.
Function :
the main function of Levatores Costarum muscles is to elevate the ribs and facilitate inspiration during breathing.
Interspinales
Interspinales muscles (Musculi interspinales);
The Interspinales muscles are short and paired muscles that connect adjacent spinous processes of the vertebral column.
These muscles are divided regionally into three parts :
interspinales cervicis
Interspinales Thoracis
interspinales lumborum
They are well developed in the cervical and lumbar parts of the spine, but may be entirely absent in the thoracic area.
Attachments of the Interspinales muscles
Interspinales cervicis
Origin:
The superior aspect of spinous processes of vertebrae C3 to T1
Insertion:
The inferior aspect of spinous processes of vertebrae C2 to C7
Interspinales Thoracis
Origin:
The superior aspect of the spinous process of vertebrae T2, T11 & T12 (variable)
Insertion:
The inferior aspect of spinous processes of vertebrae T1, T10 & T11
Interspinales lumborum
Origin:
Superior aspects of spinous processes of vertebrae L2 to L5
Insertion:
inferior aspects of spinous processes of vertebrae L1 to L4
Nerve supply :
The Interspinales muscles are supplied by the posterior rami of the respective spinal nerves.
Blood supply :
The Interspinales muscles receive blood supply from dorsal branches of respective regional arteries, namely the vertebral, deep cervical, occipital, transverse cervical, superior and posterior intercostal, subcostal, and lumbar arteries.
Function :
the function of the Interspinales is to stabilize the adjoining vertebrae of the vertebral column. They also assist in the extension of the cervical and lumbar spine.
Intertransversarii
Intertransversarii muscles (Musculi Intertransversarii);
The Intertransversarii muscles are small muscles that pass between the transverse processes of adjacent vertebrae and are most developed in the cervical and lumbar area of the spine.
Intertransversarii Colli is found In the cervical region and is composed of anterior and posterior sets.
Intertransversarii Lumborum is found in the lumbar region. They contain four pairs of muscles that extend between adjacent transverse processes of lumbar vertebrae.
Nerve supply :
The Intertransversarii Colli is supplied by the anterior and posterior rami of cervical spinal nerves, while the lumbar Intertransversarii is supplied by the anterior and posterior rami of lumbar spinal nerves.
Blood supply :
The Intertransversarii Colli receive arterial supply from the occipital, deep cervical, ascending cervical and vertebral arteries, while lumbar Intertransversarii is vascularized by the dorsal branches of lumbar arteries.
Function :
The function of the Intertransversarii Colli muscles is to help in lateral flexion and stabilization of the cervical spine. Similarly, the function of the lumbar Intertransversarii is to aid in the same side lateral flexion of the lumbar spine when acting unilaterally and to stabilize the lumbar spine when acting bilaterally.
Back Pain :
Back pain is one of the most common causes people go to the doctor or miss work, and it is a leading cause of disability worldwide.
Fortunately, you can take measures to prevent or relieve most back pain. If prevention fails, simple home treatment and proper body mechanics often will heal your back within some weeks and keep it functional. Surgery is rarely required to treat back pain.
Causes
Back pain may develop without a cause that your doctor can identify with a test or other investigation.
- Muscle strain or ligament sprain: Repeated heavy lifting or a sudden awkward movement can strain back muscles and sprain spinal ligaments.
- muscle spasm
- Bulging or ruptured disks.
- Arthritis: Osteoarthritis can affect the lower back. In some cases, arthritis in the spine can cause narrowing of the space around the spinal cord, a condition called spinal stenosis.
- Osteoporosis. Your vertebrae in the spine can develop painful fractures if your bones become porous and brittle.
- injuries, fractures, or falls
Structural problems
Structural problems may also result in back pain.
- Ruptured disks: Each spinal vertebra are cushioned by disks. If the disk ruptures there will be more pressure on a nerve, resulting in pain in the back.
- Bulging disks: In the same way as ruptured disks, a bulging disk can cause more pressure on a nerve root.
- Sciatica: A sharp and shooting type of pain travels through the buttock and down the back of the leg, caused by a bulging or herniated disk pressing on a nerve.
- Arthritis: Osteoarthritis can lead to problems with the joints in the hips, lower back, and other places. I
- Abnormal curvature of the spine: If the spinal curves in an unusual way, back pain can result. An example is scoliosis, in which the spine curves shift to the side.
- Osteoporosis: Bones, including the vertebrae of the spine, become brittle and porous, which causes compression fractures more likely.
- Kidney problems: Kidney stones or kidney infections can lead to back pain.
Other causes
- Cauda equina syndrome: The cauda equine is a bundle of spinal nerve roots that originate from the lower end of the spinal cord. Symptoms include a dull pain in the lower back and upper buttocks area, as well as numbness in the buttocks, genitalia, and thighs. There are sometimes bowel and bladder functions get disturbed.
- Cancer of the spine: A tumor on the spine may cause nerve root compression, resulting in back pain.
- Infection of the spine
- Other infections: Pelvic inflammatory disease, bladder, or kidney infections may also cause back pain.
- Sleep disorders: Individuals with sleep disorders are more likely to get experience back pain, compared with others.
- Shingles: An infection that can affect the nerve root may lead to back pain. This depends on which nerve roots are affected.
Risk factors
- Anyone can have pain in the back, even children and teens.
- Age: Back pain is more common in old age, starting around age 30 or 40.
- Lack of exercise. Weak, unused muscles in your back and abdomen might lead to pain in the back.
- Excess weight. An overweight body puts extra stress on your back.
- Diseases: Some types of arthritis and cancer can cause pain in the back.
- Improper lifting
- Psychological conditions: People prone to depression and anxiety appear to have a higher risk of back pain.
- Smoking: Smokers have increased rates of pain in the back.
- osteoporosis.
- occupational activities
- pregnancy
- a sedentary lifestyle
- poor physical fitness
- smoking
- strenuous physical exercise or work, especially if it is done incorrectly
- genetic factors
- Lower back pain is more common in women than in men, possibly due to hormonal factors.
Clinical Features :
The commonest symptom is pain anywhere in the back, and sometimes all the way down to the buttocks and legs.
Some back issues can cause pain in other parts of the body, depending on the nerve root affected.
- The pain often goes away without treatment, but if it occurs with any of the following symptoms patients should see their doctor:
- weight loss
- fever
- inflammation or swelling on the back
- persistent back pain during lying down or resting does not help
- pain down the legs
- pain that reaches below the knees
- trauma to the back
- urinary incontinence
- difficulty urinating
- fecal incontinence
- numbness around the genitals
- numbness around the anus
- numbness around the buttocks
Investigation :
- X-rays: Used to see the alignment of the bones and detect signs of arthritis or broken bones, but they are not useful for diagnosis of damage to the muscles, spinal cord, nerves, or disks.
- MRI or CT scans: Used to diagnose herniated disks or problems with tissue, tendons, nerves, ligaments, blood vessels, muscles, and bones.
- Bone scans: It is used to detect bone tumors or compression fractures caused by osteoporosis.
- Electromyography: the electrical impulses produced by nerves in response to muscles. This can confirm nerve compression, which may occur due to a herniated disk or spinal stenosis.
- The doctor may also order a blood test in case of infection.
Treatment :
Medical treatment
Medication: Nonsteroidal Antiinflammatory Drugs (NSAID). Codeine or hydrocodone, which are narcotics, may be prescribed for a short duration.
Antidepressants, such as amitriptylineTrusted Source, may be prescribed.
Surgery
- Surgery for back pain is very rare. If a patient has persistent pain and nerve compression which can lead to muscle weakness herniated disk surgery may be an option.
- Fenestration: In this operation ligamentum flavum bridging the two adjacent laminae is excised and the spinal canal at the affected level is exposed.
- Laminotomy: In addition to fenestration, a hole that is made in the lamina for wider exposure
- Hemi-laminectomy: The lamina on one side is removed.
- Laminectomy: In Laminectomy, the laminae on both sides, with the spinous process, are removed. Such a wide exposure is required for a big, central disc that produces cauda equina syndrome
Physiotherapy Treatment :
MODALITIES
Modalities offer an adjunct to evidence-based treatment in patients with Lower Back Pain.
Transcutaneous electrical nerve stimulation (TENS):
TENS, the use of electrical impulses over surface electrodes to provide symptomatic relief by modifying pain perception, has not been shown to be effective for Chronic Lower Back Pain.
Electrical stimulation:
High-voltage pulsed galvanic stimulation has been used to reduce muscle spasms and edema in patients with acute Lower Back Pain. The use of electrical stimulation typically is limited to the starting stages of treatment to allow patients to progress to more active treatments in restoring normal range of motion and strength.
Ultrasonography:
Ultrasonography is a deep-heating modality that has been shown to improve the distensibility of connective tissue and facilitate stretching. Ultrasonography is contraindicated in acute inflammatory conditions because it may worst the inflammatory response. In addition, the Ultrasonography modality is contraindicated over a previous laminectomy site.
Superficial heat:
This modality produces effects to a depth of 1 to 2 cm and has been shown to reduce pain and muscle spasms.
Short Wave Diathermy (SWD) :
Continuous Short Wave Diathermy(SWD) treatment with exercise was found to be more effective in reducing pain in patients with chronic low back pain than other treatment modalities.
Strengthening exercise :
Transverse Abdominal Contraction: Lie down on your back with both knees bent, your feet flat. contract your core muscles by pulling your belly button towards your back. Hold for 10 seconds and relax. Repeat 10 times. Perform 2 times per day.
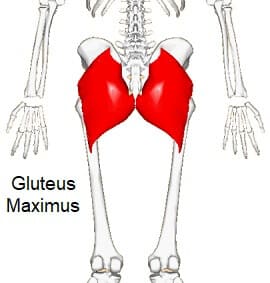
Bridging: Lie down on your back with your both knees bent. Squeeze your buttocks together then slowly lift your buttocks off the floor, keep your stomach tight and buttocks contracted. Slowly lower and release to starting position. Hold the Bridging position for 5 seconds and repeat 10 times. Perform 2 times per day.
Gluteal Squeeze: Lie down on your back with your both knees bent and squeeze your buttocks together. Hold for 10 seconds and relax. Repeat 10 times. Perform 2 times per day.
Transverse Abdominal March: Lie down on your back with both knees bent. contract your abdominal muscles by bringing your belly button toward your spine. Slowly march by lifting one leg off the ground, then alternating to the other. Continue pulling your belly button toward your spine during the Transverse Abdominal March exercise. Repeat 10 times on each side. Perform 2 times per day.
Wall Squats: Stand with your back against a wall with your feet approximately 1to 2 feet away from the wall. With feet, shoulder-width apart, squat approximately ½ of the way down, make sure that your knees do not go past your toes. Hold Wall Squats position for 10 seconds and repeat 10 times. Perform 2 times per day.
Stretching Exercise :
Child’s Pose:
This traditional yoga pose is used to stretch your gluteus maximus, thigh muscles, and spinal extensors. It helps reduced pain and tension all along your spine, neck, and shoulders.
To do Child’s Pose, follow these steps:
With your hands and knees on the floor, sink back through your hips to rest them on heels.
Hinge your hips as you fold forward, walking your hands out in front of you.
Rest your belly on your thighs.
Extend your arms in front of or alongside your body with your palms facing upward.
Focus on your breathing deeply and relax any areas of tension or tightness.
Hold Child’s Pose position for up to 1 minute.
You can do this position several times during your stretching routine.
Cat-Cow:
To do Cat-Cow, follow these steps:
Come onto all fours in a tabletop position (hands and knees on the floor).
Press into your hands and feet as you breathe in to look up, allowing your belly to fill with air.
Breath out, tucking your chin towards your chest and arching your spine toward the ceiling.
this pattern of movement Continues, moving with each breath.
Do this for 1 to 2 minutes.
Supine Hamstring Stretch: Lie on your back, starting with your both knees bent. Wrap a rope or towel around one foot of yours. While holding both ends of the towel, slowly lift one leg off the floor until a stretch is felt in the back of the leg. Hold this position for 20 seconds. Return to the starting position. Repeat 3 times on each side. Perform 2 times per day.
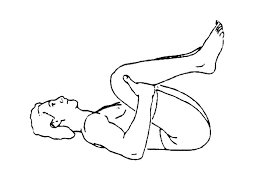
Knee to Chest: Lie down on your back with both knees bent. Grab behind one knee and gently pull the knee towards your chest until a comfortable stretch is felt in your lower back. Hold Knee to Chest: position for 20 seconds then return to starting position. Repeat 3 times on each side. Perform 2 times per day
Piriformis Stretch: Lie down on your back with both knees bent. Pull one side of your knee to your opposite shoulder. Keep your back flat, do not twist. Hold this position approx for 20 seconds then return to the starting position. Repeat 3 times on each side. Perform 2 times per day.

Prone Quadriceps Stretch: Lie down on your stomach. Put a rope, sheet, or belt around one of your feet and pull your heel toward your buttock until you can feel a stretch in the front of the thigh. Hold this position approximately for 20 seconds, then return to the starting position. Repeat 3 times on each side. Perform 2 times per day.
Calf stretch: Stand facing a wall. Keep back leg straight with heel on surface and foot facing forward. Bend the front knee slightly and lean towards the wall until a stretch is felt in the calf. It is important to keep the back heel on the surface throughout the entire stretch. Hold this position approx for 20 seconds. Return to starting position. Repeat 3 times on each side. Perform 2 times per day.

Prevention:
You might avoid pain in the back or prevent its recurrence by improving your physical condition and learning and practicing the proper mechanics of the body.
To keep your back healthy and strong:
- Exercise: increase the strength and endurance of the muscles of the back and allow your muscles to function better. Walking and swimming are good choices. Talk with your doctor regarding which activities you might try.
- Build muscle strength and flexibility. Abdominal and back muscle exercises help to strengthen muscles.
- Maintain a healthy weight. Being overweight strains back muscles. If you’re overweight, a reduction in weight can prevent back pain

9 Comments