
External Abdominal Oblique Muscle
Table of Contents
External abdominal oblique Muscle Anatomy

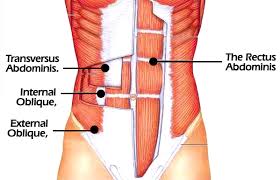
The external abdominal oblique is a paired muscle located on the lateral sides of the abdominal wall. Along with the internal abdominal oblique and transversus abdominis, it comprises the lateral abdominal muscles.
Origin
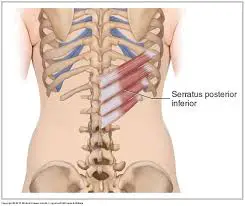
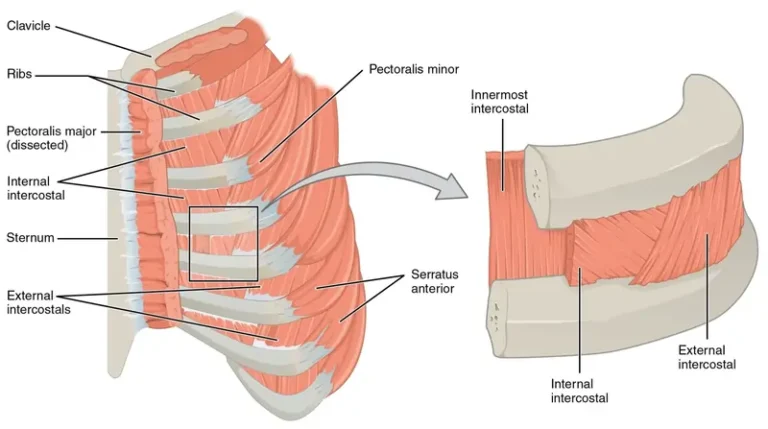
The external abdominal oblique muscle originates from the external surfaces of ribs 5-12. The attaching fibers interdigitate with those of the serratus anterior and latissimus dorsi muscle, forming a zig-zag oblique line on the lateral side of the thorax.
Insertion
The external abdominal oblique continues as an aponeurosis via which it inserts to the linea alba, pubic tubercle, and anterior half of the iliac crest.
Nerve supply
Thoracic spinal nerves T7-T12. Those are the intercostal nerves T7- T11 that supply the superior most part of the muscle and the subcostal nerve (T12) that innervates the lower part. The muscle receives sensory innervation from the lumbar plexus, via the iliohypogastric nerve (L1).
Blood supply
Blood supply to the upper two-thirds of the external abdominal oblique comes from the branches of the lower posterior intercostal and subcostal arteries, while the deep circumflex iliac artery supplies the inferior third of the muscle.
Actions:

Flexion of the torso and Contralateral rotation of the torso.
Structure of the External Abdominal Oblique Muscle
The anterior and lateral regions of the abdomen are the location of the external oblique. Its aponeurosis is located on the front wall of the belly, and its muscular portion occupies the side. It is broad, thin, and unevenly quadrilateral. Because of subcutaneous fat deposits and the tiny size of the muscle, the oblique is not visible in the majority of people.
It originates from the inferior borders and exterior surfaces of the fifth through twelfth (lower eight) ribs, each of which has eight fleshy digitations. The lower digitations are attached to the apex of the last rib’s cartilage, the intermediate digitations are attached to the ribs at a distance from their cartilages, and the upper digitations are arranged in an oblique line that runs inferiorly and anteriorly.
Between the corresponding processes of the serratus anterior muscle, the five superior serrations increase in size from above to below, while the three lower ones decrease in size from above to below and get comparable processes from the latissimus dorsi between them. The fleshy fibers travel in different directions from these attachments. Its posterior fibers create a free posterior boundary that extends from the ribs to the iliac crest.
The middle and upper fibers compose the anterior layer of the rectus sheath, directed anteriorly and inferiorly, respectively, and become aponeurotic near the midclavicular line. The lowest ribs’ insertion into the anterior portion of the iliac crest’s outer lip occurs almost vertically below. Fibers from each side of the external oblique decussates at the linea alba created this aponeurosis.
The external oblique aponeurosis forms the inguinal ligament. The inguinal canal is also influenced by the muscle.
The distance between the external and internal oblique muscles is not significant.
Function of the External Abdominal Oblique Muscle
Similar to a Valsalva maneuver, the external oblique pulls the chest lower and compresses the abdominal cavity, raising intra-abdominal pressure. Additionally, it can rotate in the opposite direction from its original position and side bend in the same direction. For example, the right external oblique can rotate to the left and side bend to the right, and vice versa. The internal oblique muscle rotates ipsilaterally but performs similar actions.
Strengthening exercise
Russian Twists
- Sit up with your legs out in front of you, knees bent and your heels on the floor, your back at a 45-degree angle to the floor. Hold a medicine ball or dumbbell (try 8 to 10 pounds) with both hands by your stomach.
- Keep your back straight and the medicine ball close to your torso as you twist to the right and left.
Sit-ups to twist:
- Lie on your back with your knees bent and feet flat on the floor.
- Place your hands behind your head, engage your core, and do a full sit-up. At the top of the sit-up, bring your right elbow to your left knee and twist your body toward that side.
- Lower back down to start.
- Repeat this movement alternating sides each time.

Side planks
- Start on your side with your feet stacked on top of each other and your bottom forearm directly below your shoulder.
- Engage your core and raise your hips until your body is in a straight line from head to toe.
- Hold this exact position without letting your hips drop for 30 seconds or more, then repeat on the other side.
Clinical Importance
Trunk flexion is less possible when there is bilateral muscle weakness, and in these situations, standing straight will show anterior pelvic tilting.
Trigger points: Incisions, physical trauma, emotional strain, increased load during exercise, or even a new training regimen can all cause the development of trigger points in the abdominal obliques. Secondary trigger points may result from other visceral pathologies. The most frequent locations of trigger points for obliques:
Pain is referred diagonally across the abdomen, groin, and genitalia from the lateral lower quadrant of the abdominal wall close to ASIS.
Pain in the upper abdomen and lower chest that is a few inches below and lateral to the sternum’s xyphoid process may be mistaken for heartburn.
Oblique strain
Baseball players frequently sustain oblique strains, especially pitchers. It can impact the trailing internal oblique or the contralateral (leading) side external oblique in both pitchers and hitters.
3 Comments