
Shoulder Joint: Anatomy, Movement, Function
Table of Contents
Shoulder Joint Anatomy
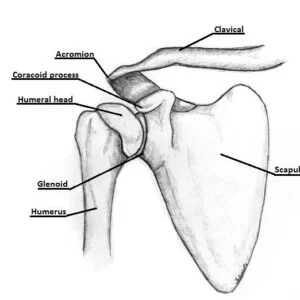
~The shoulder joint (glenohumeral joint) is a ball and socket joint between the scapula and the humerus. It is the major joint connecting the upper limb to the trunk.
~t is one of the most mobile joints in the human body, at the cost of joint stability. In this article, we shall look at the anatomy of the shoulder joint and its important clinical correlations.
~it has the greatest range of motion in any joint in the body.
Articulating Surfaces
~The shoulder joint is formed by the articulation of the head of the humerus with the glenoid cavity (or fossa) of the scapula. This gives rise to the alternate name for the shoulder joint – the glenohumeral joint.
~Like most synovial joints, the articulating surfaces are covered with hyaline cartilage. The head of the humerus is much larger than the glenoid fossa, giving the joint a wide range of movement at the cost of inherent instability.
~To reduce the disproportion in surfaces, the glenoid fossa is deepened by a fibrocartilage rim, called the glenoid labrum.
~structurally, it is a weak joint because the glenoid cavity is too small and shallow to hold the head of the humerus in place.(the head is four times the size of the glenoid cavity),this arangement permits great mobility.stability of the joint is maintained by the following factors.
- the coracoacromial arch or secondary socket for the head of the humerus.
- the musculotendinous cuff of the shoulder.
- the glenoid labrum helps in deepening the glenoid fossa.stability is also provided by the muscles attaching the humerus to the pectoral girdle,the long head of the biceps brachii,and atmospheric pressure.
Ligaments:
1.The capsular ligament:
~it is very loose and permits free movements.it is least supported inferiorly where dislocations are common. Such a dislocation may damage the closely related axillary nerve.
~medially,the capsule is attached to the scapulabeyond the supraglenoid tubercle and the margins ofthe laburm.
~laterally it is attached to the anatomical neck of the humerus with the following exceptions.
~inferiorly,the attachment extends down to the surgical neck.
~superiorly,it is defecient for passage of tendon of the long head of the biceps brachii.
~anteriorly,the capsule is reinforcedby supplemental bands called the superior ,middle and inferior glenohumeral ligaments. the capsule is lined with synovial membrane.and the extension of this membrane forms a tubular sheath for the tendon of the long head of the biceps brachii.
2.the coracohumeral ligament:
~it extends from the root of the coracoid process to the neck of the humerus opposite the greater tubercle.it gives strength to the capsule.
3. Transverse humeral ligament:
~it bridges the upper part of the bicipital groove of the humerus(between the greater and lesser tubercles)the tendon of the long head of the biceps brachii passes deep to the ligament.
4. The glenoid labrum:
~it is a fibrocartilaginous rim which covers the margins of the glenoid cavity,thus increasing the depth of the cavity.
Bursae related to the joint:
1.The subacromial bursa.
2.The subscapularis bursa,communicates with joint cavity.
3.The infraspinatus bursa,may communicates with joint cavity.
Bones of the shoulder joint
Clavicle:
~forms the front portion of the shoulder girdle, and is palpable,along its entire length with a gentle S-shaped contour.
~articulates atone end with the sternum(chest bone) and acromion of the scapula at the other(roof of the shoulder).
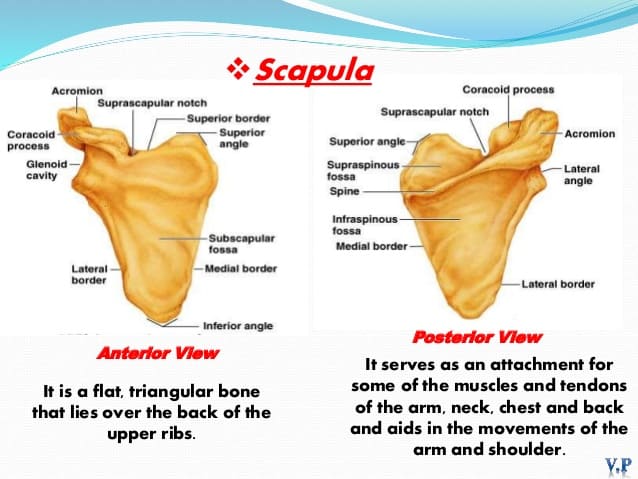
Scapula:
Proximal humerus:
~the proximal humerus consist of head ,neck , greater and lesser tubercles and shaft.
~the neck lies between the head and lesser and greater tubercles.
~the greater and lesser tubercles are prominent landmarks on humerus and serve as attachment site for the rotator cuff muscles.
Ossification centres:
Clavicle:
~it is the 1st bone to osify.
~it has no medullary cavity.
~it occurs by intramembranous ossification.
~secondary ossfication centre via endochondral.
~medial epiphysis ossifies at 12-19 yrs and fuses at 22-25 yrs.
~lateral epiphysis ossifies and fuses at 19 yrs.
Scapula:
~body and spine ossify at birth.
~coracoid process-atavastic epiphysis,centre at 1 yr, base at 10 yr.
~acromian-fuses by 22 yr via 2-5 centres at puberty.
~genoid-upper 1/4 ossify at 10 yr lower 3/4 appear at puberty,fuse by 22 yrs.
Proximal humerus:
~humeral head-ossifies at 6 months.
~greater tuberosity ossfies at 1 to 3 yrs.
~lesser tuberosity ossifies at 4 to 5 yrs.
~physis close at 14-17 yrs girls and 16-18 yrs boys.
joints of the shoulder complex:
- Glenohumeral
- acromioclavicular
- Sternoclavicular
- Scapulothoracic
*Glenohumeral Joint:
~ joint type:-Ball and socket synovial joint.
~the glenohumeral joint is the most mobile joint in the body. the socket is very shallow(glenoid fossa), and does not hold on to the ball (humeral head)very well.
~it is therefore up to a group of muscles to hold the ball in the socket providing stability and some movement. the glenoid labrum also helps to improve the stability of the shoulder.
~a glenoid labrum is a cartilage ring around the glenoid fossa. this labrum makes the socket deeper. giving it a larger and deeper contact surface to articulate with the head of the humerus.
~the articular capsule is a fibrous bag of tissue, fused with local ligaments, which provides a sealed sac around the glenohumeral joint.
Glenohumeral ligaments:
~provide anterior stability to the glenohumeral joint.
- superior (SGHL)
- middle (MGHL)
- inferior (IGHL)
*Coracohumeral Ligament:
~arises from the lateral base of the coracoid process and extends onto both tuberosities.
~it forms the bicipital tendon sheath and strengthens the capsule anteriorly.
~importance-resists inferior and posterior translation.
Transverse humeral ligament:
~bridges the upper part of the bicipital groove through which the long head of the biceps passes down.
Acromioclavicular joint:
~joint type:-plane or sliding synovial joint.
*bones involved in the articulation: ~acromion of the scapula
~distal end of the clavicle
*movements: only small translations
~anterior/posterior glide
~Superior/inferior tilt
~rotation
Acromioclavicular ligament:
~acts to secure the acromion and clavicle and provides a complete capsule around the joint.
Coracoclavicular ligaments:
~ Anchor the lateral aspect of the clavicle to the coracoid process of scapula. It consists of two small ligaments holding the scapula laterally, these are:-
*Trapezoid:-attaches to trapezoid line on the inferior surface of the clavicle.
*conoid:-attaches to conoid tubercle of the clavicle.
*joint type:-saddle synovial joint.
*bones involved in the articulation:
~manubrium of the sternum
~proximal end of the clavicle.
*movements:-
~anterior/posterior glide
~superior/inferior tilt
~rotation
*joint type:-not a true joint, but known as a pseudo joint.
*bones involved in the articulation:
~anterior surface of the scapula
~ribcage of the thorax
Scapulothoracic joint:
Movements of Shoulder Joint
The shoulder joint has the Highest range of movement (ROM) than any other joint in the Body. Joints are ball-and-socket type, which allows movements in three degrees of freedom, Movement ranges are:
- Flexion (180°) – extension (60°)
- Abduction (180°) – adduction (0°)
- Internal rotation (90°) – external rotation (90°)
A combination of all these movements gives circumduction.
Shoulder Girdle movement are :
- protraction and retraction
- elevation and depression
- anterior tilt and poterior tilt
- upward rotation and downward rotation
~as there is minimal body contact, it is up to the muscles, attaching to the scapula, and thorax to stabilize and control movement at this articulation.
~there is no joint capsule or synovial fluid.
Muscles around the shoulder joint
The scapulohumeral and thoracohumeral muscles are working to produce movement at the shoulder joint.
| Shoulder Movement | Muscle Name |
| Shoulder Flexion | Pectoralis major, deltoid, coracobrachialis, long head of biceps brachii |
| Shoulder Extension | Latissimus dorsi, teres major, pectoralis major, deltoid, long head of triceps brachii |
| Shoulder Abduction | Supraspinatus muscle, deltoid |
| Shoulder Adduction | Coracobrachialis, pectoralis major, latissimus dorsi, teres major |
| External Rotation | Teres minor, infraspinatus, deltoid |
| Internal Rotation | Subscapularis, teres major, latissimus dorsi, pectoralis major, deltoid |
*Blood supply:-
- Anterior circumflex humeral vessels.
- Posterior cicumflex humeral vessels.
- Suprascapular vessels.
- Subscapular vessels.
Nerve supply:
- Axillary nerve
- Musculocutaneous nerve
- Suprascapular nerve
Gateways to the Posterior scapular region:
~Suprascapular foramen
~Quadrangular Space
~Triangular space
~Triangular interval
*Suprascapular foramen:
~it is formed by the suprascapular notch of the scapula and the superior transverse scapular ligament which converts the notch into the foramen.
~the suprascapular nerve passes through the suprascapular foramen.
*Quadrangular Space:
~its boundaries are formed by:
~the inferior margin of the teres minor
~surgical neck of humerus
~the superior margin of the teres major
~lateral margin of the long head of the triceps brachii.
*Axillary nerve and posterior circumflex humeral artery and vein pass through this space
*Triangular space:
~its boundaries are formed by:
~the medial margin of the long head of the triceps brachii
~the superior margin of the teres major
~the inferior margins of the teres minor
The circumflex scapular artery and vein pass through this space:-
Triangular interval:
~boundaries are formed by:
~the lateral margin of the long head of the triceps brachii
~the shaft of the humerus
~the inferior margin of the teres major
The radial nerve, profunda brachii artery, and associated veins pass through it.
~the muscles and joints of the shoulder allow it to move through a remarkable range of motion.
~arm flexion(0-135)
~arm extension(45-60)
~arm abduction(0-180)
~arm adduction
~medial rotation of the arm(90)
~lateral rotation of the arm(0-90)
~cicumduction(this is a combination of the above movements)
Shoulder Joint-Related Conditions
Frozen shoulder is an Inflammation that develops in the shoulder and causes pain and joint stiffness. As a frozen shoulder progresses, Shoulder joint movement can be severely restricted.
Osteoarthritis of the shoulder are less common, age-related “wear-and-tear” arthritis that occurs in the elderly. The shoulder osteoarthritis is less often affected than the knee osteoarthritis.
Rheumatoid arthritis is a form of arthritis in which the immune system attacks the joints, causing inflammation and pain. Rheumatoid arthritis can affect any joint, including the shoulder, However, small joints such as fingers are more affected.
Gout is also a form of arthritis in which crystals form in the joints, causing inflammation and pain. The shoulder is a less common location for gout.
A rotator cuff tear is a tear in one of the four muscles or tendons surrounding the top of the humerus. A rotator cuff tear may be due to sudden injury, or result from overuse.
Shoulder impingement: The acromion (edge of the scapula) presses on the rotator cuff as the arm is lifted. If inflammation or an injury in the rotator cuff is present, this impingement causes pain.
Shoulder dislocation: The humerus or one of the other bones in the shoulder slips out of position. Raising the arm causes pain and a “popping” sensation if the shoulder is dislocated.
Shoulder tendonitis: Inflammation of one of the tendons in the shoulder’s rotator cuff.
Shoulder bursitis: Inflammation of the bursa, the small sac of fluid that rests over the rotator cuff tendons. Pain with overhead activities or pressure on the upper, and outer arm are symptoms.
Labral tear: An accident or overuse can cause a tear in the labrum, the cuff of cartilage that overlies the head of the humerus. Most labral tears heal without requiring surgery.
How Shoulder Joint examination done?
Magnetic resonance imaging (MRI scan): An MRI scanner uses a high-powered magnet and a computer to create high-resolution images of the shoulder and surrounding structures.
Computed tomography (CT scan): A CT scanner takes multiple X-rays, and a computer creates detailed images of the shoulder.
Shoulder X-ray: A plain X-ray film of the shoulder may show dislocation, osteoarthritis or a fracture of the humerus. X-ray films cannot diagnose muscle or tendon injuries.
Shoulder Treatments
Shoulder surgery: Surgery is generally performed to help make the shoulder joint more stable. Shoulder surgery may be arthroscopic (several small incisions) or open (large incision).
Arthroscopic surgery: A surgeon makes small incisions in the shoulder and performs surgery through an endoscope (a flexible tube with a camera and tools on its end). Arthroscopic surgery requires less recovery time than open surgery.
Physiotherapy treatment for shoulder pain-related condition: An exercise program can strengthen shoulder muscles and improve flexibility in the shoulder. Physiotherapy treatment is an effective, non-surgical treatment for many shoulder pain-related conditions.
Pain relievers: Over-the-counter relievers mainly NSAIDs such as acetaminophen (Tylenol), ibuprofen (Motrin), and naproxen (Aleve) can relieve most shoulder pain. More severe shoulder pain may require prescription medications.
Use of RICE Principle: RICE stands for Rest, Ice, Compression (not usually necessary), and Elevation. RICE can improve the pain and swelling of many shoulder injuries.
Corticosteroid (cortisone) injection: A doctor injects cortisone into the shoulder, reducing the inflammation and pain caused by bursitis or arthritis. The effects of a cortisone injection can last several weeks.
FAQs
The rotator cuff muscles are the main muscle group that supports the shoulder joint.
the four muscles are:
The supraspinatus
infraspinatus
teres minor
subscapularis
When the rotator cuff muscles are inserted into the proximal humerus, they combine to form a musculotendinous cuff.
The glenohumeral ligaments (superior, intermediate, and inferior)
the coracohumeral ligament are two main ligaments that connects the scapula to the humerus.
Ball-and-socket joints, like the hip and shoulder joints, permit rotation, sideways, forward, and backward motion. hinge points. The only motions possible with hinge joints, which include the fingers, knees, elbows, and toes, are bending and straightening.
The scapula, or shoulder blade, clavicle, or collarbone, and humerus, or upper arm bone, are the three bones that make up the shoulder. The acromioclavicular joint, which is formed by the acromion, the highest point of the scapula, meeting the clavicle, and the glenohumeral joint, allows movement of the shoulder.
9 Comments