Amputation Of Lower Limb: Indication, Type, Treatment
Table of Contents
Definition of Lower Limb Amputation
Lower limb amputation is the removal of a leg, foot, or toes from the body. These body parts are called extremities. Amputations are done either by surgery or they occur by trauma to the body.
Indication Of Lower Limb Amputation:
- Trauma
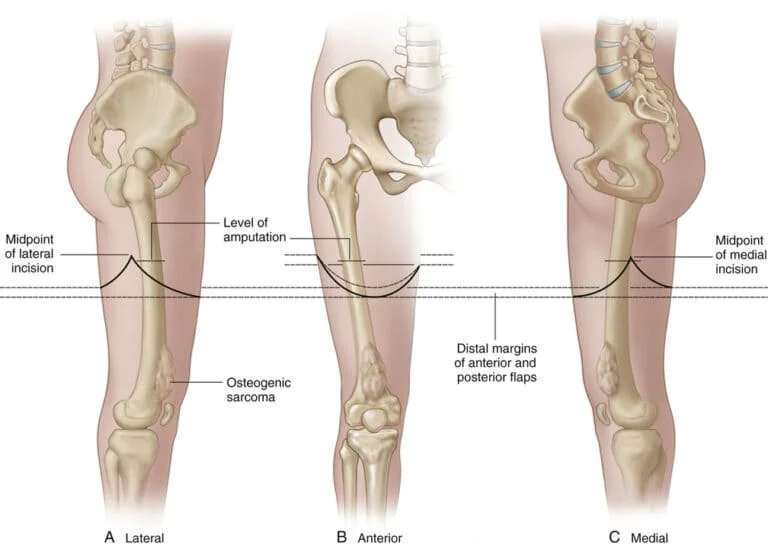
- Malignant tumors
- Nerve injuries and infections
- Extreme heat and cold
- Peripheral Vascular Insufficiency
- Congenital absence of limbs or malformations
- severe infections like gas gangrene, osteomyelitis
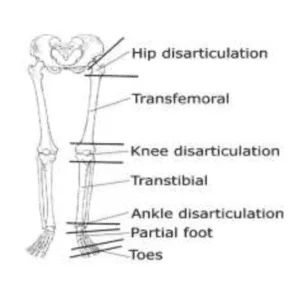
Level Of Lower Limb Amputation:
- Transfemoral (Above Knee Amputation)
- Knee Disarticulation
- Transtibial (Below Knee Amputation)
- Ankle Disarticulation
- Symes
- Partial Foot (Chopart)
- Toe amputation
Below Knee Amputation :
Definition Below Knee Amputation:
A below-knee amputation known as transtibial amputation includes the removal of the ankle joint, distal tibia, fibula, and foot with soft tissue structures. An above-knee amputation (AKA) is performed less than a below-knee amputation, it has better rehabilitation and functional outcomes. The rates of lower extremity amputation have reduced recently.

Transfemoral (Above Knee Amputation)
The Optimal Length of the trance femoral Amputation is 23 to 30 cm as measured from the tip of the greater trochanter. 7.5 cm is the minimal length for a useful stump.
Disarticulation :
Disarticulation can be done through the hip and knee as well. Knee disarticulation is cosmetically not acceptable in women as the prosthesis required is rather bulky at the knee and hence not attractive. Below the knee, amputation is generally preferred to the though knee disarticulation.
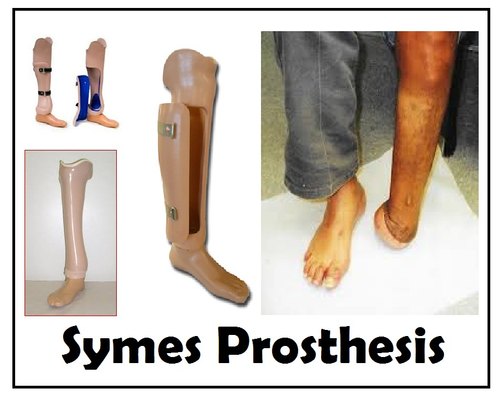
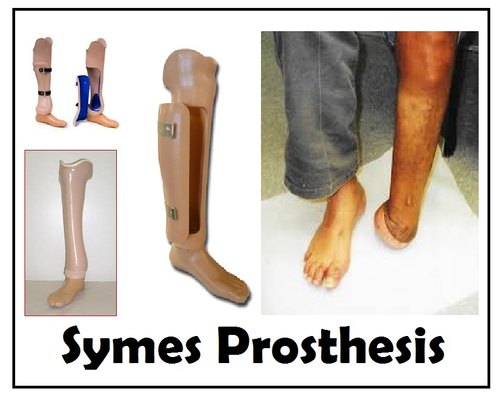
Syme Amputation:
Amputation is done at the level of the ankle joint with preservation of the heel pad. In Symes Amputation the tibia and fibula are divided above the ankle joint. The remaining skin over the heel is attached back to the end of the stump with or without a part of the calcaneum. Because of the intact heel, it becomes an end-bearing stump and the patients generally manage to walk well even barefoot after this type of amputation. Amputation through different parts of the foot has almost become ancient these days.
Toe Amputation:
It is the removal of a toe from the foot.
Causes of Toe Amputation: Vascular Disease, Diabetes, Trauma, frostbite

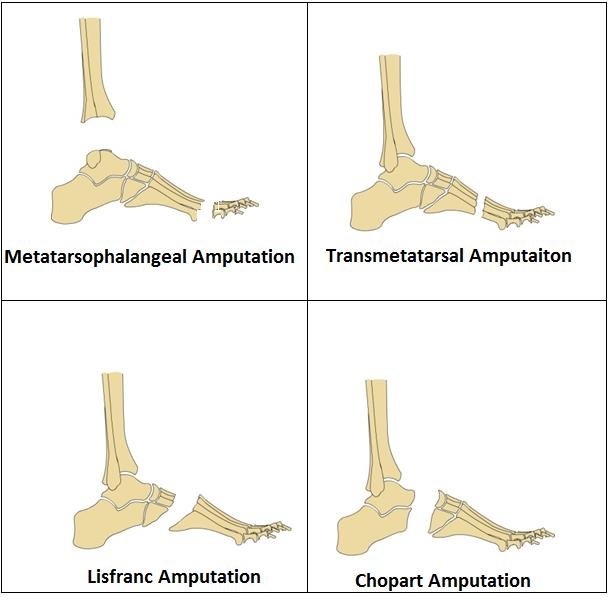
Metatarsal phalangeal disarticulation:
In Metatarsal phalangeal disarticulation, Disarticulation is performed at the metatarsal phalangeal joint.
Transmetatarsal Amputation:
It is the removal of the metatarsal from the foot.
Lisfranc Amputation:
It is the removal of the foot at the tarsometatarsal level.
Chopart Amputation:
It is a midfoot or forefoot level of amputation.
Syme Amputation:
Syme amputation is an amputation at the level of the ankle joint in which the heel pad is preserved.
Boyd’s Amputation:
In this amputation, the level of the ankle is preserved with a calcaneus and heel pad.
Multidisciplinary team:
- The management of complex diabetic foot complications requires the involvement of various members comprising the specialist team in order to provide comprehensive management of multiple aspects of diabetes care.
- diabetologist
- podiatrist
- microbiologist
- nurse
- orthopedic surgeon
- vascular surgeon
- Physiotherapist
Physiotherapy Treatment For Lower Limb Amputation :
Physiotherapy treatment: physiotherapy treatment is required Before surgery and also postoperatively.
Before Surgery:
Before your surgery, your physical therapist may Prescribe exercises according to the conditions before the operation, and to improve the flexibility and strength of the hip and knee Physiotherapist teach you how to walk with a walker or crutches and Educate you about the procedure
Preoperative Training Programm:
- Prevention of thrombosis by maintaining the circulation by the movement of limbs.
- Prevention of chest complications by deep breathing, coughing, and postural drainage preserves the mobility of all joints and Improves mobility of other areas like a trunk, pelvis, shoulder girdle
- Teach the patient, how to position the limb in bed
- Teach the patients how to transfer, monitoring of wheelchair,single-leg standing, and balancing
- Psychological reassurance has an important role in the recovery of amputation.
Early postoperative stage :
- To check the efficiency of Preoperative training
- Prevent chest complications and thrombosis
- Prevention of contracture and deformities:
- the common contracture is knee flexion contracture
- contracture is prevented by proper positioning of the amputated limb passive movement of a limb
- Maintenance of strength and mobility
- The patient can be encouraged to move in the bed by pushing up the body on the arms.
- This push-up exercise has the advantage of strengthening the muscles in the upper limb which is necessary for using ambulation aids later on.
- strengthening exercise should be given to the whole body except the joint proximal to amputation.
Management of the stump:
Improper management of stumps is one of the common causes of delayed rehabilitation.
Surgical trauma is one of the common causes of stump edema, it may occur because of bad bandaging, associated degenerative joint disease, poor venous return, diabetes, and kidney disease.
How to control edema of the stump:
Stimulation of limb in elevation with an elastic bandage. Resisted exercise of the stump and other joints.
stump bandaging and conditioning:
Bandaging plays an important role in conditioning and shaping the stump by reducing edema of the stump. 4-inch elastic bandage for below-knee amputation is used. The bandage should be removed during exercise.
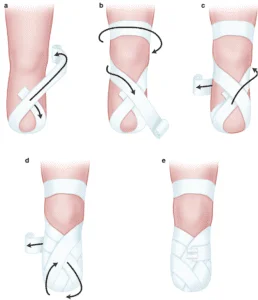
Principles of bandaging the stump:
The pressure of the bandage should be moderately firm and distributed evenly
Extra pressure is necessary at corners to obtain the conical shape of the stump. pressure should be decreased proximally.
Diagonal, oblique, or spiral turns should be used during bandaging.
The below-knee stump should be bandaged with knee slight flexion.
An above-knee stump should be bandaged with the position of the hip in extension and adduction.
Intermittent variable air pressure machine:
This machine is also called a controlled air pressure machine. It is used to control edema by improving the circulation of blood and lymph.
Shrinker socks:
edema can be treated with elastic socks.
Rigid dressing: A rigid plaster of Paris dressing is given to the young patient. It also reduced edema.
Stump hygiene:
Stump hygiene includes regular washing of the stump with warm disinfected water soap and after drying the part. The patient should be educated on protecting the areas and positions of the affected limb.
After removal of Stitches :
When the stitches are removed and the suture line healed, the most important is stump conditioning.
stump conditioning :
An ideal stump is perfectly healed, firm, conical, and with minimal flabby tissues.
Bandaging: pressure and application should be proper during bandaging.
Exercise:
Isometric exercise for muscles of the stump, which originated above the joint proximal to the amputation.
Massage :
massage can be helpful for improving the tone of the muscles.
Stimulation:
Electrical stimulation with the stump elevation is used to reduce edema and improve muscles tone.
Pressure:
Exposing the stump to pressure by either early use of pylon or gradual training of bearing weight on the terminal weight-bearing area of the stump. This can be done by providing a soft cushion and adjusting the height of the stool in the parallel bars.
Mobility Stage:
this is a stage of mobilization and restoration of functional independence. It starts with crunch walking. Elderly patients may need initial ambulation practice in the parallel bar.
Mobilization and strengthening exercise :
Mobilization of the body segment proximal Amputation.
Proprioceptors neuromuscular facilitation techniques, Progressive resistive exercise, and strong endurance exercise to the specific muscles groups are needed to facilitate effective body function with the prosthesis.
Below knee amputation: Hip abductors, and extensors Knee Extensors, And Flexors.
Above-knee amputation: Hip Flexion, abductors, Flexors, and shoulder girdle muscles.
Symp Amputation: Knee Extensors, Flexors, Hip abductors, and extensors.
Complications Of Lower Limb Amputation:
- Excess bleeding
- Blood clots
- Edema
- Poor healing
- Deep vein thrombosis (DVT)
- wound infection
- pneumonia
- phantom limb” pain
- depression
- Stump ulceration
- Flap necrosis
- Joint stiffness
- Osteomyelitis
- Osteoporosis
Prosthesis For Lower Limb Amputation:
Prosthesis For Above Knee Amputation :
The prosthetic design:
Socket:
Quadrilateral H-type socket, in which most of the weight of the body is transmitted through the ischial seat and then the posterior brim of the socket.
Suspension: Suspension with a double swivel pelvic band with a multiaxial joint provides all hip joint movements. However, a rigid pelvic band only allows flexion, and extension is preferred in cases where muscle control and stability are deficient. A suction socket with a valve or modular prosthesis is the alternative method of the Above Knee Prosthesis.
Knee Mechanism:
Hand-operated or semi-automatic locking mechanism along with constant friction device or knee joint with a free mechanism in which swing can be given.
Feet.Uniaxial or multiaxial SACH foot is preffered.It stimulates plantar flexion through compression of the rubber heel. The uniaxial foot allows both dorsiflexion and plantarflexion. The biaxial foot also allows inversion and eversion. The foot made of wood molded with plastic material is incorporated with rubber bumpers to provide necessary movements of joints.
Prosthesis For Below-knee Amputation :
Two types of Prosthesis used For Below Knee Amputation:
1) Conventional Prosthesis
2)Patellar tendon-bearing Prosthesis
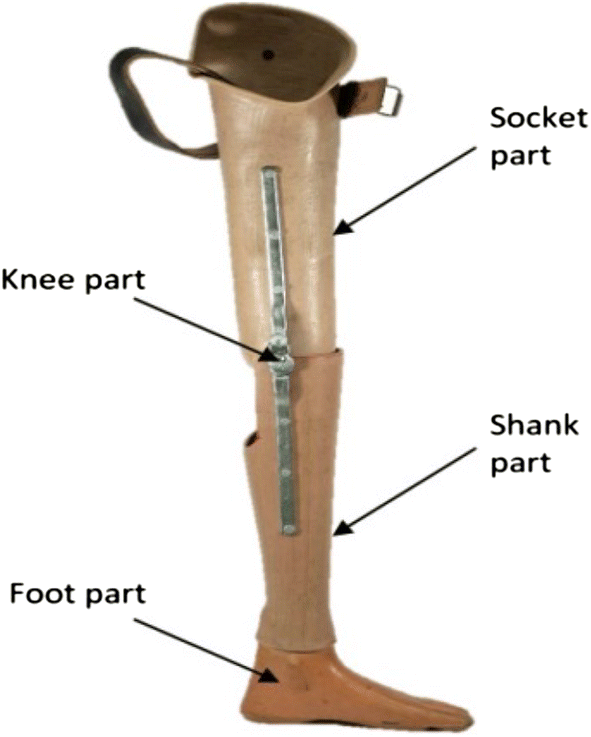
1) Conventional Prosthesis :
- conventional Prosthesis with thigh corset. It is preferred by the patient with,
- An unstable knee joint
- Flexion deformity of knee joint more than 25 degrees
- Very short stump
- Anesthetic stump
- Patellar malformation
- Patients with heavy-duty
Part of the Conventional Prosthrosis are :
- Thigh Corset
- Socket
- Suspension
- Knee Joint
- Feet
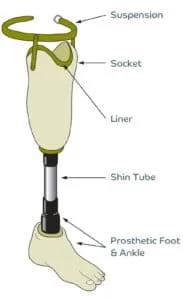
2)Patellar Tendon Bearing(PTB)Prosthesis:
The Patellar Tendon Bearing(PTB)Prosthesis is ideal and handy for patients with a long stump. offer normal gait patterns and early Rehabilitation to the patient.
Part of the Patellar Tendon Bearing(PTB)Prosthesis are :
- Socket
- Weight-bearing areas
- Weight relieving areas
- Suspension
- Feet
Prosthesis for foot:
Structurally, prosthetic feet can be divided into two types of groups: First with a rigid connection to the prosthetic shank (non-articulated) and Second with a hinged ankle
mechanism(articulated). By function, prosthetic feet can be divided into the following groups:

- Solid Ankle Cushioned Heel (SACH)
- Elastic (flexible) Keel Foot
- Single-Axis Foot
- Multi-Axis Foot
- Dynamic-Response Foot
- Microprocessor Foot.
Prosthesis For Symes Amputation:
Toe Prosthesis: