Clavicle Fracture
Table of Contents
What is a Clavicle Fracture?
A clavicle fracture is a break in the collarbone, one of the main bones of the shoulder. This type of fracture is fairly common, accounting for about 5% of all adult fractures.
The majority of clavicle fractures occur as a result of the bone snapping or breaking from a fall onto the shoulder or an outstretched arm. A broken collarbone can be excruciatingly painful and make the movement of your arm difficult.
Many clavicle fractures can be treated by using a sling to immobilize the arm and shoulder while the bone heals. However, when some clavicle fractures occur, the bone fragments move far out of place. In these more complicated fractures, surgery may be required to realign the bones.
Anatomy
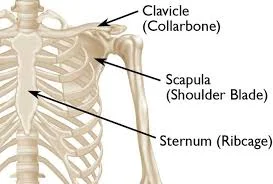
The clavicle is situated between the sternum (ribcage) and the scapula (shoulder blade). It’s the bone that connects the arm to the rest of the body.
The clavicle is located above several vital nerves and blood vessels. However, when a fracture occurs, these vital structures are rarely harmed.
The clavicle is the bone that connects the sternum (breastplate) to the shoulder. It is a very solid bone with a slight S-shape that is visible in many people. It connects to the sternum via a cartilage joint known as the sternoclavicular joint. At the other end, the bone meets the shoulder area at the acromion of the shoulder blade (scapula). The acromioclavicular joint is the cartilage-containing joint at the end of the bone.
The collarbone serves as a strut between the sternum and the shoulder blade. Due to the clavicle’s critical location, any severe force on the shoulder, such as falling directly onto the shoulder or falling on an outstretched arm, transfers force to the clavicle. As a result, one of the most commonly broken bones in the body is the collarbone.
Causes of the Clavicle Fracture
Among the most common causes for a broken collarbone are:
- falls; like landing on an outstretched arm or shoulder.
- Sports-related injuries include strikes to the shoulder sustained directly on a field, rink, or court.
- accidents involving vehicles, such as bicycles, motorcycles, or cars.
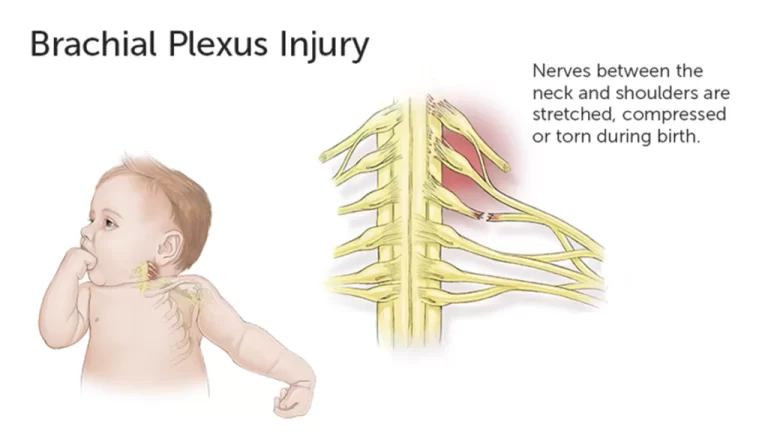
- birth injury, usually as a result of a challenging vaginal birth.
Mechanism of injury
Younger people are more likely to sustain these injuries as a result of moderate to high-energy mechanisms such as car accidents or sports injuries, whereas the elderly are more likely to sustain injuries as a result of a low-energy fall.
Although a fall onto an outstretched hand was once thought to be the most common mechanism, it has been discovered that the clavicle most frequently fails in direct compression caused by a force applied directly to the shoulder. A clavicle fracture is caused by a direct fall onto the lateral shoulder in approximately 87% of reported cases.
Classification of the Clavicle Fracture
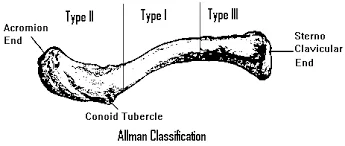
Clavicle fractures are typically described using the Allman classification system, which divides the clavicle into three groups based on location and was later revised by Neer (in which Group II was further classified into three types).
- Group I: Fractures of the middle third or midshaft (the most common location),
- Group II: Fractures of the lateral third. A common non-union location.
- Group III: Fractures of the medial third
Robinson’s classification was more specific for middle-third fracture patterns, whereas Craig’s classification was more specific for lateral-third fractures.
Symptoms of the Clavicle Fracture
If you break your collarbone, you may experience the following symptoms:
- When the bone breaks, it makes a snapping or grinding sound.
- Sharp pain that worsens when you move that area.
- Because the bone no longer supports the shoulder, it slumps down or forward.
- Difficulty moving or lifting the arm, possibly with a grinding sensation.
- There may be bruising, swelling, or tenderness in the affected area.
- A visible bump through the skin.
- Numbness or “pins and needles” (rarely).
- Bone poking through the skin, occasionally causing bleeding.
Diagnosis
History and Physical examination
- The uninjured arm can be used to cradle the injured extremity.
When an injury occurs, a patient may report hearing a snapping or cracking sound.
The shoulder may appear shortened and droopy in comparison to the opposite side. - Over the clavicle, swelling, inflammation, and tenderness may be observed.
- Abrasion over the clavicle is possible, indicating that the fracture was caused by a direct mechanism.
- Gentle manipulation may reveal crepitus caused by the fractured ends rubbing against each other.
- Breathing difficulties or decreased breath sounds on the affected side may indicate a pulmonary injury, such as a pneumothorax.
- A concomitant injury may be diagnosed by palpating the scapula and ribs.
- Tenting and blanching of the skin at the fracture site can suggest an upcoming open fracture, which requires surgical stabilisation most of the time.
Nonuse of the affected side’s arm is a neonatal symptom.
A brachial plexus injury is confirmed by associated distal nerve dysfunction. - A subclavian artery injury may be indicated by decreased pulses.
- A subclavian venous injury is indicated by venous stasis, discolouration, and swelling.
A client’s history and physical examination are frequently used to make a diagnosis.
Acromioclavicular joint injury, rib fracture, scapular fracture, shoulder dislocation, rotator cuff injury, and sternoclavicular joint injury are all possible diagnoses for a clavicle fracture.
Complications of clavicle fractures, such as pneumothorax, brachial plexus injury, and subclavian vessel injury, must also be thoroughly evaluated.
Depending on the severity of the trauma, laboratory studies are ordered on clavicle fractures. When a vascular injury is suspected, obtain a complete blood count (CBC) to determine haemoglobin and hematocrit levels. Perform an arterial blood gas (ABG) test and obtain an expiration posteroanterior (PA) chest film if a pulmonary injury is suspected or identified. Other imaging studies that can be used to evaluate a clavicle fracture are as follows:
- clavicle and shoulder radiography
- Scanning with computed tomography (CT) and 3-dimensional (3-D) reconstruction
- Arteriography
- Ultrasonography
Treatment of Clavicle Fracture
Non Surgical Treatment
You may not need surgery if the broken ends of the bones have not shifted significantly out of place. Many broken collarbones can heal on their own.
Nonsurgical options include:
Arm assistance. A simple arm sling is usually used for immediate comfort and to keep your arm and shoulder in place while the injury heals.
Medication. Pain relievers, such as paracetamol, can help as the fracture heals.
Therapy for the body. Although there will be some discomfort, it is critical to keep your arms moving to avoid shoulder and elbow stiffness. Often, patients will begin doing elbow motion exercises immediately after the injury.
Following a clavicle fracture, it is common to lose some shoulder and arm strength. Once the bone begins to heal, your pain will decrease and your doctor may begin gentle shoulder exercises to help prevent stiffness and weakness. You will gradually begin more strenuous exercises once the fracture is completely healed. Follow-up care. You must see your doctor regularly until your fracture heals.
Complications. A clavicle fracture can move out of place before it heals in some cases. You must see your doctor regularly to ensure that the bone remains in place.
When a fracture does not heal, it is called a nonunion.
In some cases of nonunion, the patient has very little pain and good motion, requiring no further treatment.
In other cases, nonunion can cause significant pain and may necessitate surgery to repair.
A malunion occurs when the fracture fragments move away from the place and the bones heal in that position. Surgical treatment for this is extremely rare and is determined by how far the bones are out of place and how much this affects your arm movement.
A large bump may form over the fracture site as it heals. This usually diminishes over time, but a small bump is often permanent.
Surgical treatment
If the broken ends of the bones have shifted significantly out of place, your doctor may advise surgery.
Typically, surgery consists of repositioning the broken bone fragments and preventing them from moving until they heal. When you’ve recovered, this can help you regain shoulder strength.
Internal fixation and open reduction. This is the most common method of treating clavicle fractures. The bone fragments are first repositioned (reduced) into their normal alignment during the procedure. The bone fragments are then secured with special metal hardware.
Screws and plates. The bone fragments are held in place with special screws and metal plates attached to the bone’s outer surface after being repositioned into their normal alignment.
You may notice a small patch of numb skin beneath the incision after surgery. You may be able to feel the plate through your skin because the clavicle is directly beneath the skin.
Unless they are causing pain, plates and screws are not routinely removed after the bone has healed. Hardware issues are uncommon, but some patients report that seatbelts and backpacks irritate the collarbone area. If this occurs, the hardware can be removed once the fracture heals.
Screws or pins. After the bone ends have been replaced, pins or screws can be used to keep the fracture in place. Incisions for pin or screw placement are typically smaller than those for plate placement.
Pins and screws frequently irritate the skin where they are inserted and are typically removed after the fracture has healed.
Rehabilitation
Rehabilitation. Exercise will help you regain movement and strengthen your shoulder. Your doctor may recommend that you work with a physical therapist or provide you with a home therapy plan.
Typically, therapy programmes begin with gentle motion exercises. As your fracture heals, your doctor will gradually add strengthening exercises to your programme.
Although it is a slow process, adhering to your physical therapy plan is critical to returning to all of your favourite activities.
Protection of the Clavicle Fracture
Until clinical union is achieved, the patient’s shoulder is immobilised in a sling or figure-of-eight brace. A figure-of-eight brace is commonly thought to prevent or reduce secondary fracture shortening during the healing process. However, it is associated with more discomfort and pain, including nerve compression with temporary brachial plexus palsies and venous blood return restriction.
Furthermore, studies concluded that there are no differences in healing time or nonunion rate between these two techniques for treating clavicle fractures. As a result, a sling is usually used, and internal rotation immobilisation is usually recommended for 2-4 weeks. Unless for exercise and personal hygiene, wear the sling during the day. It is the patient’s choice whether to wear it at night or not, but they must exercise caution.
Summary
The clavicle is a bone that connects the sternum to the shoulder and is located between the sternum and the scapula. It is one of the most commonly broken bones in the body, accounting for about 5% of all adult fractures.
Common causes of clavicle fractures include falls, sports-related injuries, accidents involving vehicles, and birth injuries. The Allman classification system is used to describe clavicle fractures, which can cause snapping or grinding sounds, sharp pain, difficulty moving or lifting the arm, bruising, swelling, tenderness, a visible bump through the skin, numbness, and bone poking through the skin.
Symptoms include snapping or grinding sounds, pain, drooping shoulder, swelling, inflammation, tenderness, abrasion, breathing difficulties, palpation of the scapula and ribs, tingling, and venous stasis.
Diagnosis involves a client’s history and physical examination, and complications like pneumothorax, brachial plexus injury, and subclavian vessel injury must be evaluated. Laboratory studies, such as clavicle and shoulder radiography, CT scans, and ultrasonography, can be used to evaluate clavicle fractures.
A clavicle fracture can be treated non-surgically, using arm assistance, medication, and therapy. Nonunions can cause minimal pain and good motion, while malunions can cause significant pain and necessitate surgery. Surgical treatment involves repositioning broken bone fragments and preventing them from moving until they heal. Common methods include internal fixation and open reduction, screws and plates, and pins or screws.
Rehabilitation involves exercise to regain movement and strengthen the shoulder. A sling or figure-of-eight brace is usually used until clinical union is achieved, but it is associated with more discomfort and pain. Both techniques have no differences in healing time or nonunion rate.
FAQs
The middle third segment of the clavicle is the most common site of fracture because its weakest point is at the junction of the middle and lateral thirds of the clavicle.
The most common clavicle fractures occur in the middle of the bone’s shaft, roughly halfway between the sternum and the AC joint. The most common treatment for fractures in the middle is immobilisation with a sling or a special bandage known as a figure-of-8 splint.
Malunion, or when the clavicle fracture heals with angulation, shortening, or a poor cosmetic appearance, is the most common complication of clavicle fractures.
Because the supraclavicular nerve is so close to the clavicle, it is especially vulnerable to injury during clavicle fractures and surgical treatment of these fractures.
A fall onto the lateral shoulder is the most commonly reported mechanism. Less common mechanisms include a direct blow to the clavicle or a fall on an outstretched hand. The patient may have a visible or palpable deformity over the fracture site on physical examination.
The Clavicle, also known as the collar bone, is a long bone with a sigmoid shape that forms the front part of the shoulder. It is located between the sternum and the shoulder blade.
References:
- Clavicle Fracture (Broken Collarbone) – OrthoInfo – AAOS. (n.d.). https://orthoinfo.aaos.org/en/diseases–conditions/clavicle-fracture-broken-collarbone/
- Clavicle Fractures. (2021, August 8). Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/clavicle-fractures
- Broken collarbone – Symptoms and causes – Mayo Clinic. (2022, December 10). Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/broken-collarbone/symptoms-causes/syc-20370311
- Professional, C. C. M. (n.d.). Broken Collarbone (Clavicle Fracture). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/16874-broken-collarbone-clavicle-fracture
- Clavicular Fracture. (n.d.). Physiopedia. https://www.physio-pedia.com/Clavicular_Fracture