
Iliopsoas Muscle
Table of Contents
Introduction
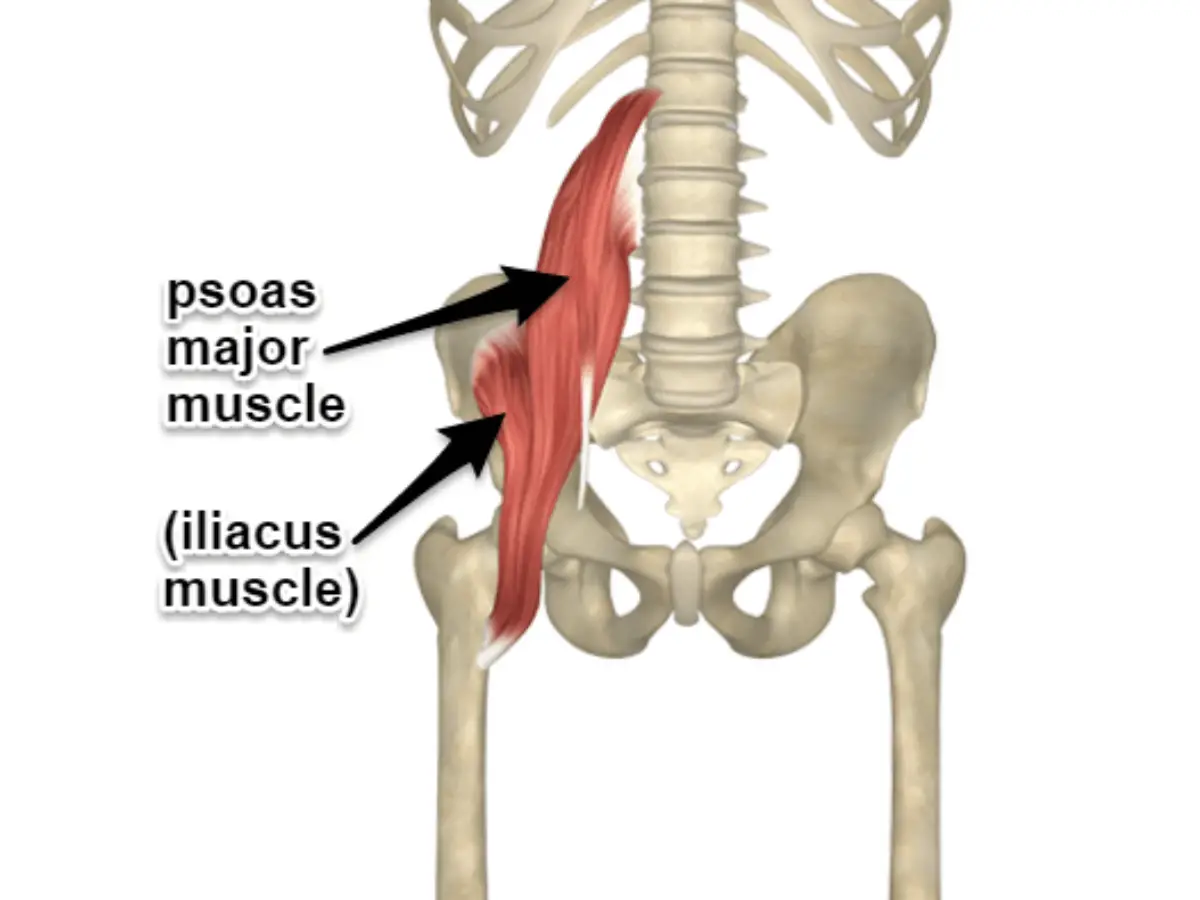
The iliacus and psoas major muscles combine to form the iliopsoas, a large complex muscle of the inner hip. Other muscles of the inner hip besides the iliopsoas are the quadratus femoris, piriformis, superior and inferior gemellus, obturator externus, and psoas minor.
The psoas major section of the iliopsoas originates from the twelfth thoracic and all five lumbar vertebrae, while the iliacus portion mostly arises from the pelvic iliac fossa. The iliopsoas have a broad origin. Around the pelvic brim, their fibres unite into a single muscular belly. A tendon that enters into the femur’s lesser trochanter marks the termination of the iliopsoas.
The primary hip flexor is the iliopsoas muscle. The psoas major can create extra movements of the lumbar vertebral column because of its proximal attachments, in addition to the joint actions of the iliacus and psoas major that produce hip flexion.
Iliopsoas muscle Anatomy
Psoas major Muscle
Located lateral to the spinal column on the posterior abdomen wall is the large and strong Psoas major muscle. It comes from the anterolateral sides of the bodies of the T12–L5 vertebrae, the intervening intervertebral discs, and the transverse processes of all lumbar vertebrae. The muscle moves inferiorly in the direction of the pelvic apex.
The lateral fibres of the psoas major combine with the iliacus fibres to produce the big iliopsoas muscle, which is situated prior to it entering the anterior thigh and crossing the border of the pelvis. The unified fibres then go to the inguinal ligament posteriorly and the hip joint capsule anteriorly. A component of the femoral triangle floor is made up of the inferior portion of the iliopsoas below the inguinal ligament. The iliopsoas finally come together to form a tendon that connects to the lesser trochanter of the femur.
The anterior rami of the lumbar spinal nerves, primarily L1 and L2, with little input from L3 and L4, innervate the psoas major. Its obturator and lumbar arteries, as well as branches of the external iliac and femoral arteries, all contribute to its blood supply, which is mostly supplied from the iliolumbar branch of the internal iliac artery.
Iliacus Muscle
The superior two-thirds of the iliac fossa, the iliac crest, and the lateral face of the sacrum give birth to the triangular-shaped iliacus muscle. The anterior sacroiliac and iliolumbar ligaments, which join the pelvis to the spinal column, are the source of some extra muscle fibres. The iliacus origin extends anteriorly in the iliac fossa compared to the anterior superior and anterior inferior iliac spines .. Here, the iliacus gets a little slip of muscle called the iliocapsularis, which originates from the top region of the hip joint capsule.
The iliacus muscle then combines with the most lateral psoas major fibres to produce the iliopsoas muscle, which inserts into the lesser trochanter of the femur after passing anterior to the hip capsule. A sizable subtendinous iliac bursa, which occasionally interacts with the joint cavity, divides the iliopsoas tendon from the hip joint.
The femoral nerve’s L2, and L3, branches innervate the iliacus. It is supplied with blood from the lumbar, obturator, external iliac, lumbar, and iliolumbar branches, just as the psoas major.
Structure and Function
The main flexor of the thigh that has the capacity to augment and extra-rotate the coxofemoral joint is the iliopsoas musculotendinous unit (IPMU). The iliopsoas muscle contraction flexes and tilts the trunk from the side of the contraction if the latter is stationary.
Each muscle may function independently. The psoas major muscle stabilizes the lumbar spine while sitting and the thigh flexion in a supine or standing position. The iliacus muscle stabilizes the pelvis and permits proper hip flexion during running. During the initial 15 degrees of movement, the psoas major stabilizes the femoral head in the hip acetabulum. The iliac fascia may be stretched by the psoas minor muscle, which also helps in trunk flexion.
Three muscles make up the iliopsoas musculotendinous unit: the iliacus, psoas major, and psoas minor.
Lying posteriorly at the level of the retroperitoneum, the iliopsoas musculotendinous unit is a component of the posterior abdominal wall and the
inner muscles of the hip.
The psoas major, which includes the vertebral body and the transverse process of the last thoracic vertebra, has a fusiform shape and arises from the lateral surfaces of the bodies of the first four lumbar vertebrae. There are intervertebral discs along the way as well. The iliac muscle bundles are located in the iliac fossa, which is reached by the muscle bundles pointing downward and parallel to the lumbar vertebrae. The inguinal ligament is passed beneath by the bundles of the iliac and psoas major muscles. They attach to the femur’s tiny trochanter using a strong tendon. In general, the size of the right muscle is larger than that of the left.
The psoas minor muscle, which originates from the final thoracic vertebra and the first lumbar, is situated in front of the main psoas muscle and is found in 60% to 65% of people. For 90% of the population, it converges with the iliac fascia and the psoas major tendon in a distal direction to enter into the iliopectineal eminence. This muscle should facilitate the iliopsoas muscle’s activity.
The lateral portions of the sacral bone wing and the top two-thirds of the iliac fossa are the sources of the fan-shaped iliacus muscle. Its bundles cross in front of the hip joint and beneath the inguinal ligament. The lesser trochanter and the major psoas muscle tendon combine with the iliac muscle’s muscular bundles. The iliac muscle’s lateral little fibres, referred to as the infratrochanteric muscle, increase the iliac muscle’s surface area in contact with the iliac bone.
Fascia
Numerous anatomical linkages exist between the iliopsoas musculotendinous unit and the fascial system that surrounds it. The IPMU fascia joins the chest fascia (endothoracic fascia) superiorly and the diaphragm muscle’s arcuate ligament posteriorly.
The IPMU fascia unites anteriorly with the fascia covering the kidneys, pancreas, inferior vena cava, descending aorta, ascending and descending colon, duodenum, and cecum colon.The IPMU fascia inferiorly fuses with the pelvic floor fascia and the fascia lata of the thigh; the fusion with the latter links the psoas fascia to the fascial system of the abdominal muscles. It unites with the quadratus lumborum muscle’s fascia posteriorly.
Embryology
The iliopsoas muscles’ embryological development has not been well studied. From the paraxial mesoderm, the iliopsoas musculotendinous unit (IPMU) is formed. The musculature is created after eight weeks of gestation and a three-centimeter embryo. Most likely, the tendinous portion that connects the three muscles that makeup IPMU forms inside the eventual inguinal ligament.
Blood Supply and Lymphatics
The most significant artery for the muscle’s blood supply is the external iliac artery, which is derived from the common iliac and delivers blood branches to the iliacus muscle along its path. The common iliac artery produces thin branches that feed blood to the psoas major and minor muscles.
The external iliac vein, which is an extension of the femoral vein, gathers blood from the iliacus muscle and the psoas major and minor muscles.
The external iliac lymphatic plexus, which will eventually merge into the common iliac plexus, is the lymphatic system that supplies the iliopsoas muscle.
Nerve Supply
The psoas major and minor muscles are innervated by the short collateral branches of the lumbar plexus (L1-L3), whereas the iliacus muscle is innervated by the femoral nerve, also known as the terminal nerve of the lumbar plexus (L1-L4).
Muscles
The majority of the primary muscle fibres in the psoas in a human model are anaerobic, or IIA fibres (approximately 60%), with the remaining portion being aerobic, or type I fibres (about 40%). The origin and insertion of the muscle affects its dispersion. More red fibres are seen at the lumbar level (origin), while more white fibres are found at the hip joint. This indicates that while it has a more dynamic function at the hip level, its function at the lumbar level is more static (posture).
The percentages of the aerobic and anaerobic fibres in the psoas minor muscle are comparable in an animal model. Furthermore, an increasing proportion of the main fibres in the iliacus muscle are of the anaerobic IIB type, as they approach the hip joint.
Physiologic Variantions
The scientific literature contains several anatomical variants of the iliopsoas muscle.
The iliacus muscle and the psoas major muscle unite to form the iliopsoas tendon. Recent research found that a large number of people will detect a bilateral bifid tendon (two tendons) at the level of the femur’s lower trochanter (approximately 26%). A very tiny proportion of instances have bilateral bifid tendons, and there are also extremely few cases with three tendons present. The tendon may be the source of discomfort and hip joint dysfunction, as will be demonstrated later. There may be additional muscle or auxiliary bodies in the psoas major muscle, which is mostly on the left and innervated by lumbar branches. Although the psoas major muscle belongs to just one muscle, it might appear to have several fascicles.
The iliacus muscle has anatomical variations. In particular, on the left, there may be a supernumerary iliacus; it would originate from the middle third of the iliac crest, detached from the major iliacus muscle but consistently innervated by the femoral nerve and with insertion associated with the tendon of the iliopsoas complex. The femoral nerve innervates the iliacus minimus muscle, also known as the iliocapsularis, an accessory muscle that may begin at the iliolumbar ligament, travel in front of the iliacus muscle, lateral to the psoas major muscle, and ultimately merge into the muscle fibres of the iliopsoas complex.
There may be differences in the innervation that impact the iliopsoas complex. Normally, the femoral nerve and the lumbar plexus run behind the psoas major muscular. The psoas major muscle may occasionally be penetrated by the lumbar plexus, resulting in the typical clinical signs of nerve entrapment. The iliacus muscle may be crossed by the femoral nerve.
Surgical Considerations
Psoas Abscesses
The existence of an abscess in the psoas major muscle body is an uncommon incidence but warrants aspiration. The reasons are various, including the closeness to visceral and lymphatic tissues, which can infiltrate the muscle and infect the contractile structure. Other predisposing factors are the existence of diabetes, intravenous use of medications, renal failure, HIV, and direct trauma with hematoma. The existence of an abscess in the muscle might offer clinical indications such as back discomfort, groin pain, pain in the hip, and fever; it is more prevalent in males than in women. Generally, the infecting agents may be Staphylococcus aureus, streptococci, or Escherichia coli. Computed tomography and blood testing are necessary for a proper diagnosis; abscess drainage and ultimate necrotic tissue cleanup are necessary for therapy.
Impingement of the Iliopsoas Tendon
The iliopsoas complex tendon and other nearby soft tissues may be beaten by the prosthetic head’s movement during hip extension after femoral head replacement surgery. The surgeon may choose to examine the area between the tendon and the femoral head in this instance. 4.3% of treatments involving total replacement of the coxofemoral joint may result in an impingement of the iliopsoas and associated discomfort as well as a functional reduction in mobility.
Iliopsoas Bursitis
Its cause is not fully understood, but bursitis involving the iliopsoas complex tendon is an inflammation that increases the bursa’s volume and causes pain when moving. It may be the consequence of prior hip surgery, inflammatory arthritis, trauma, or overuse of the tendon during sporting activities. As for the resolution, aspirating more fluid while introducing corticosteroids and anesthetic is the treatment. Ultrasonography confirms the diagnosis.
Additional Surgical Intentions
Distal tenotomy surgery is used in the pediatric population when there are significant contractures and stiffness (such as cerebral palsy and other neurological illnesses). With this method, walking becomes easier and the youngster may adopt an independent stance. Masses of muscular tumors are seldom removed.
Iliopsoas Muscle Exercise
Iliopsoas Muscle Strengthening Exerciser
Knee to chest

To perform this stretch, take a supine position on the floor and extend your legs.
The left knee should be bowed gently towards the chest.
Keep your back flat and bring your left knee as near your chest as possible without feeling uncomfortable.
Squeeze the glute and extend your right leg as far as you can.
It holds for ten to fifteen seconds.
Go back to the beginning and repeat with the other leg
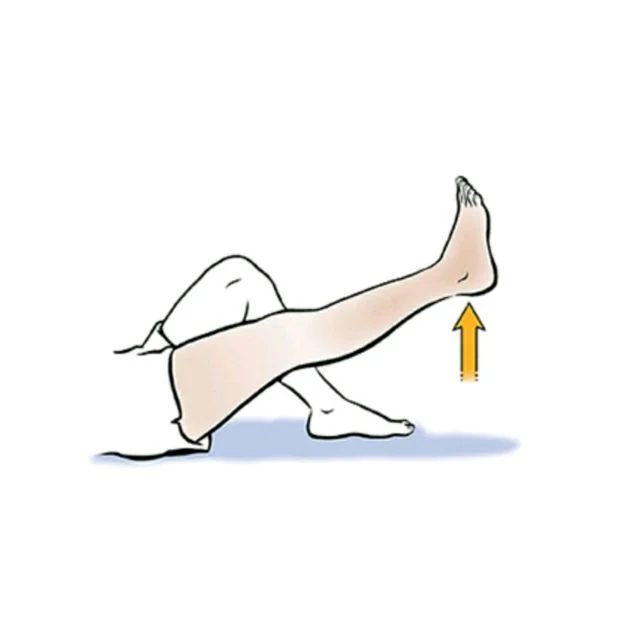
Straight Leg Raise (SLR)
The patient is placed in a supine position while one leg is straight and the other leg is slightly bent.
Tighten your quadriceps to stabilize the muscles on your straight leg.
Take a slow breath and raise the straight leg six inches off the floor
For three seconds hold.
With a controlled exhale, drop the leg to the floor.
Relax and repeat 10 times more
Frankensteins
Start in a standing position with your arms extended shoulder-level in front of you.
Place your weight on one side.
Then move the leg to the other side while maintaining the leg straight and the knee completely extended. Lift your leg as high as you possibly can comfortably.

Depending on your range of motion, you might be able to touch your hands to your toes.
Hold on just only two seconds. Release your leg then and return to the starting position.
When you have completed repeating the other leg relax.
For thirty repetitions, alternating between the left and right sides.
Iliopsoas muscle stretching exercise
Standing Hip Flexor Stretch

Those who find it difficult to bend over might benefit from this stretch.
How to Stretch: Place your feet about hip distance apart and stand tall.
Put the left foot forward to assume the split position.
Tuck the pelvis and use your core muscles. The hands may be placed on the patient’s left leg.
Lean the left leg forward gradually while keeping the rear leg straight.
The right side of the patient’s thigh, groin, and front hip may all feel stretched.
Assume a lunge position and hold it for 20-30 seconds. There shouldn’t be any low back ache for the individual. Release the strain if you do.
Return to the beginning posture gently and switch sides.
Stretch your hip flexors two to three times on each side while standing.
Hip Flexor Bed Stretch

The best way to perform this stretch is to lie on your back on the bed with your left leg closest to the edge.
Drop the left leg slowly over the bed.
With the foot resting on the bed, the right leg may remain bent.
The hip flexor is stretched, and the patient is aware of this.
The foot should ideally not contact the ground, but rather hover over it. However, as long as it touches the ground, it’s fine.
Bend the knee carefully to deepen the stretch. The front of the hip and the length of the thigh should be felt by the person.
Hang there for a duration of 20 to 30 seconds.
Return to the bed’s left leg and turn it so that the right side is closest to the edge.
Stretch your hip flexors two to three times on each side.
Clinical Significance
The iliopsoas muscle lies close to several viscera, and some conditions affecting the muscle might mimic illnesses of the internal organs. An appendicitis-like pain is experienced in the lower right quadrant when there is a right muscle lesion. Muscle hypertrophy may obstruct the colon’s fecal material from passing through it correctly.
The genitofemoral nerve at the level of the vessel’s lacuna gap (lacuna vasculorum), below the inguinal ligament, and the femoral nerve and the lateral cutaneous nerve of the thigh at the level of the lacuna musculorum may be compressed as a result of this.
The complicated iliopsoas make it challenging to detect a single issue, however, the following will provide several diagnostic techniques for spotting repeated dysfunctions.
Iliopsoas Hematoma
One may develop a hematoma in the iliopsoas muscle spontaneously or as a result of direct trauma. The latter may result from mistakes made in blood coagulation control (prior cardiac valve operations), hemophilia, or liver illness (cirrhosis). Other potential reasons include little, underappreciated injuries, improper muscle fiber healing during physical activity, and broken small blood vessels. One of the signs is an unexpected backache that isn’t brought on by effort or discomfort in the flank (the side of the affected muscle). Grey Turner sign, a visible ecchymosis on the flank due to a big retroperitoneal hematoma, compression of the femoral nerve with involvement of the thigh, and leg muscle hypoesthesia can all happen.
Iliopsoas Snapping
Following a thorough history (about half of IS cases follow hip trauma) and a comprehensive palpatory examination
A malfunction of the iliopsoas complex known as iliopsoas snapping (IS) or coxa saltans produces audible and palpable noise during vigorous hip motions, either with or without pain. IS comes in three flavors: intra-articular, internal, and external. The external kind is caused by the iliotibial band, whereas the noise and discomfort are caused by the gluteal maximus muscle tendon, which involves tendons moving over the great trochanter.
The internal form is characterized by exostoses of the small trochanter or movement of the iliopsoas complex tendon along the anterior capsule of the femoral head, including the iliopectineal eminence (muscle pulley). Moving internal bodies, labral tears, synovial chondromatosis, and the existence of persistent subluxation (in dancers or youngsters) are the causes of the intra-articular type.
The active iliopsoas snapping test is carried out with a thorough history (about 50% of IS cases follow hip trauma) and a broad palpatory examination to identify any irregularities. Placing the patient supine in the Fabere test posture, the operator applies pressure to the inguinal region. After abduction, external rotation, extension, and rest, the patient brings the lower limb back to its neutral position. Palpation often reveals the presence of discomfort, particularly at 30 to 45 degrees of flexion, as well as a characteristic noise, however, this may not always be the case.
Iliacus Muscle Hematoma
The iliacus muscle hematoma is an uncommon occurrence. Similar to the psoas major muscle, blood coagulation disorders, whether inherited or acquired, can result in hematoma. The symptoms, which include discomfort in the belly, groin, and hips as well as weakness in the quadriceps muscle, might come on following trauma or surgery. Other symptoms include tachycardia, hypovolemia, and in more severe cases, a drop in hematocrit levels.
Facioscapulohumeral Muscular Dystrophy
The iliopsoas muscle was shown to be less affected by facioscapulohumeral muscular dystrophy in 67% of patients using magnetic resonance imaging studies, and the illness progressed more slowly in these individuals’ course. Over time, the patient’s muscle tone and size remain consistent, but their neuromuscular coordination is compromised, especially while walking. Other dystrophies (dystrophinopathy) also exhibit these features.
Groin Pain
Iliopsoas tendinitis, which may have resulted from prior surgery or functional overloads, can cause discomfort in the groin area. It is commonly advised to do an endoscopic iliopsoas tenotomy in the first instance and to lessen the muscle’s workload in the second.
Other Issues
Physiotherapy techniques are part of the conservative treatment for iliopsoas snapping
The primary strategies during the acute period are rest and anti-inflammatory medications. The patient will be shown several exercises, such as iliopsoas complex stretching, active and passive hip joint mobilization, and posture-improving lumbar lordosis exercises after the treating physician recommends physiotherapy.
When there is a weakening of the psoas major muscle or any other muscle involved in the movement of the hip, lower leg, or lumbar area, muscular strengthening is necessary. It is advised to perform exercises in front of a mirror to enhance the caliber of neuromotor intervention. After a rehabilitative course, the motor function should normally return pain-free in 6 to 12 months.
Knee discomfort may result from compression of the femoral nerve caused by the iliopsoas muscle. The patient should practice stretching exercises to lessen the tension produced by the muscle before choosing surgical therapy to release the femoral nerve.
In most cases, if the patient can adhere to the PT recommendations, surgery can be avoided. The British Medical Acupuncture Society states that acupuncture for the iliopsoas muscle is a viable alternative therapy.
Osteopathic manual treatment can help physiotherapy by acting on deep muscle-articular regions using gentle procedures that have no adverse effects or by reducing pain, especially in the post-surgical stages.
FAQ
Your hip joint’s main flexor is the iliopsoas muscle. It is composed of the iliacus, psoas major, and minor. Together, these muscles allow you to flex your hip and stabilize your lower back and hips when you run, walk, or get out of a chair.
A sharp, stabbing pain that is felt in the hip crease in the front. a sound or sensation that clicks or snaps as you bend your hips, or raise your knee. Sharp discomfort when standing or sitting, especially after a significant period of time spent sitting. Pain when jogging, walking, and sports, particularly those requiring jumping and kicking.
At the lesser trochanter, the iliopsoas connect to the femur. It serves as the hip’s strongest flexor. muscles of the thigh and hip. The lumbar spinal nerves L1–L3 (psoas) and portions of the femoral nerve (iliacus) supply the iliopsoas muscle.
The thick iliac fascia envelops the iliopsoas muscle, which is formed at the distal end by the union of the psoas and iliacus muscles. The femur’s lesser trochanter is where the common tendon is attached. When the muscle contracts, the femur rotates externally and is abducted.
Often known as the iliopsoas muscle. This complex network of muscles can act as a single entity or as distinct muscles. It is necessary for maintaining proper lumbar posture when sitting or standing, for stabilizing the coxofemoral joint, and for walking and running.
One of the muscles in the thigh’s anterior compartment is the iliopsoas. It is made up of the iliacus and psoas major, two distinct muscles. These muscles originate in the pelvis, go into the anterior compartment of the thigh under the inguinal ligament, and eventually unite to create a single tendon.
One Comment