
Rotator Cuff Muscles: Supraspinatus, Infraspinatus, Teres minor, Subscapularis
Table of Contents
Introduction :
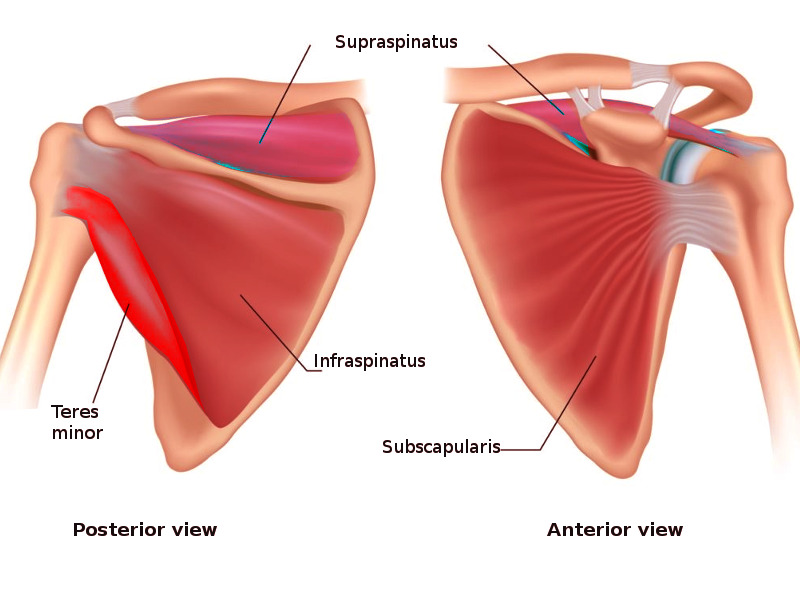
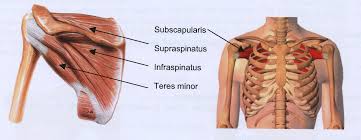
The Rotator Cuff (RC) is a common name for the group of 4 distinct muscles and their tendons, which provide strength and stability during movement of the shoulder complex. The Rotator Cuff muscles arise from the scapula and connect to the humerus head, forming a cuff around the glenohumeral (GH) joint.
The rotator cuff muscles include 4 muscles:
- 1)Supraspinatus
- 2)Infraspinatus
- 3)Teres minor
- 4)Subscapularis
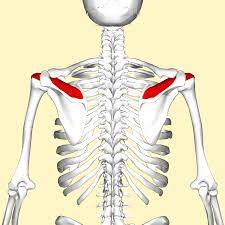
1)Supraspinatus:
The supraspinatus muscle is one of the musculotendinous support structures called the rotator cuff that surrounds and encloses the shoulder. It helps to resist the inferior gravitational forces placed across the shoulder joint due to the downward pull from the weight of the upper extremity.
Origin:
Supraspinatus fossa of the scapula. A shallow depression in the body of the scapula above the spine of the scapula.
Insertion:
Greater tuberosity of the humerus, superior facet.
Nerve Supply:
Suprascapular Nerve, C5 & 6, the superior trunk of the brachial plexus.
Blood Supply:
Suprascapular Artery.
Action:
It abducts the arm from 0 to 15 degrees, when it is the main agonist, then assists the deltoid to produce abduction beyond this range up to 90 degrees.
Internal Rotation of Glenohumeral joint
2)Infraspinatus:
Description:
The Infraspinatus muscle is a thick, triangular shape of muscle; one of the 4 muscles which comprise the Rotator Cuff of the shoulder joints.
Origin:
infraspinatus fossa of the scapula
Insertion:
The posterior aspect of greater tuberosity of the humerus, and the capsule of the shoulder joint.
Nerve Supply:
Suprascapular Nerve (C5 & C6)
Blood Supply:
Suprascapular and circumflex scapular arteries.
Action:
the Infraspinatus muscles are the external rotator of the shoulder joint.
It assists in producing shoulder extension.
With the arm fixed, abduction of the inferior angle of the scapula.

Teres Minor:
Description:
Teres Minor is a narrow muscle above teres major and triceps brachii. Teres Minor lies below infraspinatus muscles, and deep into the deltoid muscles. It is one of the four muscles which make the Rotator Cuff.
Origin:
The origin of Teres Minor is the upper two-thirds of the lateral border of the scapula.
Insertion:
Greater tubercle of the humerus
Nerve Supply:
The axillary nerve C5, C6
Blood Supply:
The Arterial Supply of teres minor muscles is a circumflex scapular artery and the posterior circumflex humeral artery.
Action:
External rotation of the shoulder joint.
It assists in the adduction and extension of the shoulder joints.
During the humerus is stabilized, abduct the inferior angle of the scapula.

Subscapularis:
Description :
subscapular fossa of the scapula is a origine of subscapularis muscle. The “subscapularis” means under the scapula. The subscapularis muscle is a triangular-shaped largest muscle.
In the rotator cuff muscle, the subscapularis is the largest and strongest muscle.
Origin:
Medial two-thirds of the subscapular fossa.
Insertion:
The fibers form a tendon that inserts into the lesser tuberosity of the humerus
Nerve Supply:
Upper and lower subscapular nerves (C5-C6) are innervated by a posterior cord of the brachial plexus.
The subscapularis is innervated by both the upper and lower subscapular nerves which come from the posterior cord of the brachial plexus. The upper part of the subscapularis muscle supply by the upper subscapular nerve, while the lower subscapular nerve branches into two, with one branch supplying the lower part of the subscapularis muscle.
Blood Supply:
Subscapular artery.
Action:
The primary function is the internal rotation of the shoulder joint. It helps in shoulder adduction and extension in some positions.

Rotator cuff muscle tear :
Rotator cuff muscles tears occur when tendons pull away from the arm bone. A tear may result from repetitive use or another injury.
Ellman Classification of Partial-Thickness Rotator Cuff Tears
Grade Description
I < 3mm (< 25% thickness)
II 3-6 mm (25-50%)
III > 6 mm (>50%)
causes of rotator cuff tear :
A trauma, such as a fall down, can cause a broken collarbone or dislocated shoulder that tears the rotator cuff muscles.
Most commonly, rotator cuff tears occur over time as the tendon wears down with aging and use (degenerative tear). People over 40 are most commonly involved.
Causes of degenerative tears include:
Bone spurs: Bony growths form on the top of the shoulder bone. These bone spurs rub against the tendon when you lift your shoulder. This shoulder impingement produced friction between the bone and tendon. Eventually, a partial or complete rotator cuff muscles tear may occur.
Decreased blood flow: Blood flow to the rotator cuff muscles is reduced as you get older. Your muscles and tendons need a healthy blood supply for repair. If blood doesn’t nourish the tendons, they may tear.
Overuse: Repetitive shoulder movements during sports activity or on the job can stress muscles and tendons, causing a tear.
risk factors for rotator cuff tears :
Anyone can experience a rotator cuff muscle tear. These factors may increase your risk:
Family history of any shoulder problems or rotator cuff injuries.
- Poor posture.
- Smoking.
- Being age 40 or older.
- Degenerative tears are most common among people who do the same repetitive shoulder movements, such as:
- Carpenters.
- Mechanics.
- Painters.
- Recreational and professional athletes who play tennis, softball, and baseball or are part of a rowing crew.
Clinical features :
- pain during raising your arm
- Difficulty in raising arm
- swelling
- Popping or clicking sounds or sensations during moving your arm.
- pain in the Shoulder worsens at night or when resting your arm.
- Shoulder weakness
- struggling to lift items
Investigation :
- Magnetic resonance imaging(MRI): Magnetic resonance imaging is a noninvasive imaging modality that is extremely sensitive and specific. It can be used to detect the size, location, and characteristics of rotator cuff muscles pathology. In a rotator cuff muscle tear, the tendon demonstrates a bright signal on T1-weighted images that increases significantly on T2-weighted images.
- X-ray: An X-ray is used to check for arthritis or bone spurs.
- ultrasound: An ultrasound to look for tendon tears.
Special Test :
Drop arm test
The drop arm test is used to assess for full-thickness rotator cuff tears, particularly of the supraspinatus muscle. This can be useful when diagnosing sub-acromial pain syndrome (shoulder impingement) or to differentiate between shoulder and rotator cuff pathologies.
The drop arm test can be more accurate when used in a battery of tests such as:
empty/full can test,
external rotation lag sign
internal rotation lag sign
Hornblower’s sign
Performing a battery of tests will help to differentiate between rotator cuff muscles and will give a more accurate diagnosis.
Technique :
Stand behind the seated patient and passively abduct the patient’s arm to 90 degrees and full external rotation, while supporting the arm at the elbow
Release the elbow support and ask the patient to slowly lower the arm back to neutral.
Interpretation :
The test is negative if the patient is able to control the lowering of the arm slowly and without any symptoms occurring.
Drop arm test is positive if there is a sudden dropping of the arm or weakness in maintaining arm position during the eccentric part of abduction, there may also be pain present during lowering of the arm, suggesting a full-thickness tear to the supraspinatus
Empty Can Test
Purpose :
The Empty Can Test is used for the assessment of the supraspinatus muscle.
Technique :
The patient’s position during the test is standing or sitting. The patient’s shoulder should be elevated to 90 degrees in the scapular plane, with the elbow extended full internal rotation and pronation of the forearm. This results in a thumbs position being downward as if the patient were pouring liquid out of a can. The therapist should stabilize the shoulder by applying a downwardly directed force to the arm, the patient tries to resist this motion. This test is considered positive if the patient experiences pain or weakness in the arm.
Medical Treatment :
Nonsteroidal anti-inflammatory drugs (NSAIDs) help to reduce pain and swelling.
Steroid injections to ease pain and swelling.
Physiotherapy treatment :
Rice Therapy
The rest of the therapy during the healing process is based on the RICE therapy, which includes:
- Rest,
- Ice treatment
- Compression
- Elevation
The basic aims and objectives of physiotherapy include :
- Prevention
- Prevention of further damage
- Restoration of function
Preventive measures
To avoid its occurrence :
- Avoid sudden lifting of heavyweight
- Avoid repeated compression of the tendon
- The age group prone to degenerative changes needs extra caution while attempting these movements with weights.
- Strengthening of rotator cuff muscles by Progressive resisted exercise. Avoid sports
Prevention of further damage
Positioning during standing: Even hanging the beam by the side of the body for a longer period puts a constant strain on the rotator cuff muscles.to prevent this we can use the support of a good arm should be taught or an arm sling with proper and secure support to the shoulder and elbow may even be considered.
Positioning during exercise: In the presence of a rupture, the patient should be taught the correct positions and actions so that the ruptured tendon is avoided exposure to any further stretch and injury. movements of the shoulder especially flexion and abduction against gravity or resistance should be discontinued; They should be initiated in a gravity eliminated position.
Passive full range of motion of the shoulder to avoid adhesive capsulitis is to be kept in mind and taught to the patient as self-assisted movements in a supine lying position and not in a standing or sitting position.
Restoration of function :
During the starting phase of an acute episode :
- Rest with proper support of a sling
- Movement of the elbow, forearm, wrist, and hand are performed
- Cryotherapy, TENS, Ultrasound therapy
After acute symptoms are abated. Isometric contraction should be given to all the three muscle groups with special emphasis on abductors and flexors with self-built-up pain-free controlled contractions.
Transverse friction massage just below the acromion is useful.
Deep heating modalities like short wave diathermy could be given to the patient.
Exercise program:
Relaxed passive movements :
Relaxed passive full-range movements with the patient in supine lying for abductors and si9de lying for flexors should be begun at the earliest. care should be taken to secure total relaxation and proper stabilization, especially during the abduction. The aim is to achieve a full range of motion without further injury to the rotator cuff.
Active or active-assisted exercise :
This program is of vital importance in the return of function. The optimal strength of the cuff muscles is the guiding principle to plan exercise. However, initiation of abduction, rotation, and flexion of the arm has to be started with gravity eliminated positions.
with the patient in the supine position, the arm is held in a neutral position of rotation with an elbow in flexion. Stabilization is given just above the glenohumeral joint over the shoulder girdle. The patient is then asked to do abduction of the arm. If the patient can perform this, the lever arm is lengthened by extending the elbow joint. The therapist should be taught the patient to perform movements without elevating the shoulder girdle. If both these movements are not possible, assisted abduction should be started with the physiotherapist totally supporting the weight of the arm. During this maneuver, the elbow is held in flexion, and the shoulder girdle is stabilized with the other arm. Rotation should be initiated in sitting and flexion in a side-lying position. This regime should be gradually progressed to abduction and flexion against gravity.
Resisted exercise :
In last, the manual resistance or resistance with dumbells starting with minimal weight could be added. it needs to be compared with the normal side to assess the progress. Properly controlled resisted program for rotator cuff muscles and self-generated tension are important because the scapular muscle; es are the powerhouse of the shoulder movements whereas the muscles of the humerus are primarily oriented to provide a greater range of motion.

44 Comments