
Muscle Hypertrophy
Table of Contents
What Is Muscle Hypertrophy?
Muscle hypertrophy refers to the process of increasing the size of skeletal muscle fibers through the enlargement of individual cells.
The process of developing larger skeletal muscles through an increase in the size of their constituent cells is known as muscle hypertrophy or muscle development.
Sarcoplasmic hypertrophy, which emphasizes greater muscle glycogen storage, and myofibrillar hypertrophy, which emphasizes greater myofibril size, are the two elements that lead to hypertrophy. It is the main objective of bodybuilding-related endeavors.
Types of Muscle Hypertrophy
There are three basic types of muscular hypertrophy:
Myofibrillar hypertrophy is the rise in the number of myofibrils, the lengthy fibers in the muscle that aid in contraction. The muscle becomes denser and stronger as the number of myofibrils rises
Sarcoplasmic hypertrophy is the term used to describe the muscles’ increased production of sarcoplasmic fluid, a fluid that contains a range of chemicals that are energy-containing.
Myostatin-related muscle hypertrophy causes a dramatic decrease in body fat and an increase in muscle mass, up to double that of normal. In addition, individuals with this illness typically possess stronger muscles than the ordinary person.
Functions Of Muscle Hypertrophy
The functions of the muscular system are:
Mobility
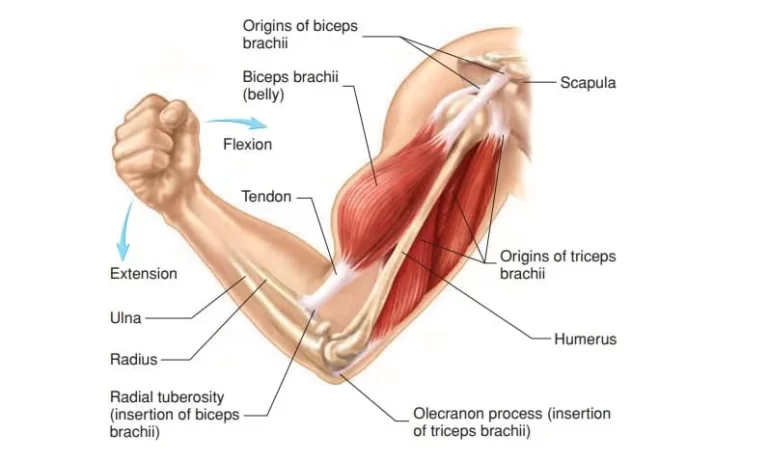
The primary purpose of the muscular system is to provide movement. Muscle contractions are a part of both fine and gross movement.
Large, coordinated motions are referred to as gross movement, and they comprise:
- walking
- running
- swimming
Smaller motions are included in fine movements, like:
- writing
- speaking
- facial expressions
This kind of movement is generally the result of the smaller skeletal muscles.
The majority of a person’s muscular action is controlled consciously. Nonetheless, certain actions are reflexive, like taking a hand away from a hot source.
Stability
Tendons of muscles wrap around joints and help maintain joint stability. Stabilization depends heavily on the shoulder and knee joints’ muscle tendons.
The muscles in the belly, back, and pelvis are known as the core muscles. They help in actions like lifting weights and stabilizing the body.
Posture
Skeletal muscles support an individual’s ability to maintain proper posture whether sitting or standing. We call this stance.
Strong, flexible muscles are essential for proper posture. Tight, weak, or stiff muscles can lead to bad posture and bodily misalignment.
Chronic poor posture causes discomfort in the shoulders, back, neck, and other joints and muscles.
Circulation
One muscle that circulates blood throughout the body is the heart. The heart contracts on its own when it receives electrical signal stimulation; it is not subject to cognitive control.
A further factor in the movement of blood throughout the body is the smooth muscle found in the veins and arteries. In the event of blood loss or dehydration, these muscles keep the blood pressure and circulation stable.
When engaging in vigorous activity, when the body needs more oxygen, it enlarges to improve blood flow.
Respiration
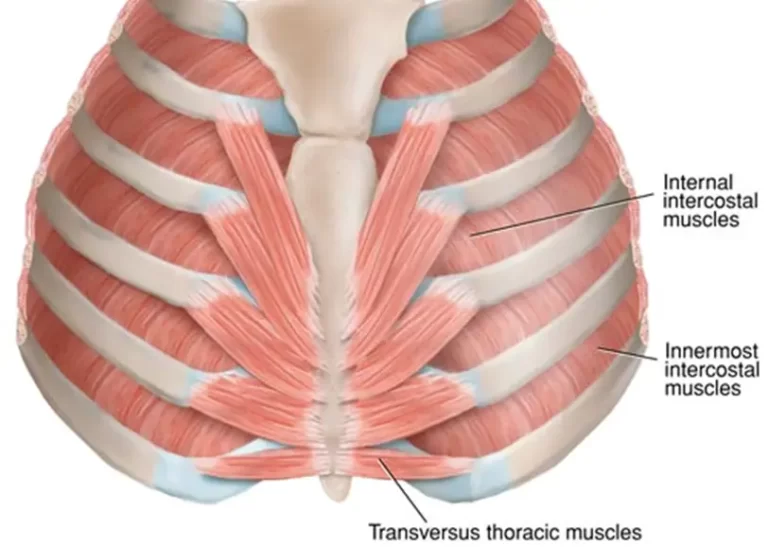
The diaphragm muscle is used for breathing.
Beneath the lungs lies a muscular dome called the diaphragm. The diaphragm pulls downward during contraction, expanding the chest cavity. Air then fills the lungs. The diaphragm muscle forces air out of the lungs as it relaxes.
The muscles in the back, neck, and belly must cooperate for someone to breathe more deeply.
Digestion
Digestion is regulated by smooth muscles in the gastrointestinal system. The mouth to the anus is the length of the GI tract.
The wave-like movement of food through the digestive tract is known as peristalsis. Food is forced into the stomach and esophagus by the contraction and relaxation of muscles in the walls of these hollow organs.
Food particles are mixed with stomach acid and enzymes by the lower muscles of the stomach while the top muscles relax to let food pass through.
Peristalsis transports the food that has been digested from the stomach into the intestines. Further contractions of muscles result in the passage of food out of the body as stool.
Urination
The skeletal and smooth muscles of the urinary system include those in the following areas:
- bladder
- kidneys
- prostate
- ureters
- urethra
Urine cannot be held in the bladder or released without the cooperation of the muscles and nerves.
Urinary issues, such inability to regulate the bladder or pee retention, are brought on by injury to the nerves that provide the muscles with impulses.
Childbirth
During birthing, the smooth muscles in the uterus flex and expand. The baby is forced into the vagina by these motions. Additionally, the pelvic floor muscles aid in directing the head of the newborn down the delivery canal.
Vision
The movements of the eye are controlled by six skeletal muscles. These swiftly contracting muscles enable the eye to:
- maintain a stable image
- scan the surrounding area
- track moving objects
A person’s eyesight may be affected if their eye muscles sustain injury.
Organ protection
The torso’s muscles guard the body’s internal organs, which are located in the front, sides, and rear. Additional protection is given by the ribcage and spine bones.
Because they lessen joint friction and absorb trauma, muscles help shield the bones and organs.
Temperature regulation
Maintaining the body at a proper temperature is one of the muscles’ major jobs. Muscle contractions account for around 85% of the heat that an individual produces in their body.
Skeletal muscles contract more vigorously to generate heat when body temperature drops below ideal levels. One manifestation of this system is shivering. To keep the body warm, blood vessel muscles also contract.
It is possible to return body temperature to normal by relaxing the smooth muscle in the blood vessels. Through the skin, this movement produces more heat and improves blood flow.
Hypertrophy stimulation
Muscle cells can expand in volume in response to a variety of stimuli. These alterations are the result of an adaptive reaction meant to improve force production or fatigue resistance in anaerobic environments.
Strength training
The capacity of an athlete to produce force through voluntary muscular contraction increases as a result of strength training (also known as resistance training), which results in neurological and muscular adaptations: Following a period of early neuro-muscular adaptation, the muscle tissue grows by producing more non-contractile components such as sarcoplasmic fluid and contractile parts called sarcomeres.
Progressive overload, which is the practice of gradually increasing resistance or repetitions throughout subsequent training sessions to maintain a high degree of effort, can cause muscular hypertrophy.
The specific processes, however, remain unclear; the prevailing theories now posit a mix of muscle injury, metabolic exhaustion, and mechanical strain.
In competitive bodybuilding and strength sports like powerlifting, American football, and Olympic weightlifting, muscular growth is crucial.
Anaerobic training
As opposed to concentrating on increasing strength, power, or endurance, the best strategy to specifically achieve muscle growth is still up for debate.
However, it was previously thought that regular anaerobic strength training would eventually lead to hypertrophy in addition to its effects on muscular strength and endurance.
Strength training and other short-duration, high-intensity anaerobic workouts can promote muscular hypertrophy.
Longer-term, lower-intensity aerobic exercise often does not produce particularly effective tissue hypertrophy; instead, endurance athletes promote neovascularization and the storage of lipids and carbohydrates in the muscles.
Temporary swelling
Muscles momentarily enlarge due to increased blood supply to metabolically active regions during exercise.
Transient hypertrophy is the term for this condition, which is also more popularly called becoming “pumped up” or “a pump.”
Muscles enlarge as a result of an inflammatory reaction two hours after an exercise and usually for seven to eleven days when tissue damage is healed.
Changes in muscle structure that are more persistent lead to longer-term hypertrophy.
Factors affecting hypertrophy
Muscle hypertrophy can be influenced by dietary factors, exercise variables, and biological factors (including sex and DNA).
Genetic variations among individuals explain a significant amount of the variation in current muscle mass. It was estimated using a conventional twin research design (like those used in behavioral genetics) that approximately 53% of the variance in lean body mass and approximately 45% of the variable in muscle fiber percentage are heritable.
In males, hypertrophy happens more quickly throughout puberty. In the late teens, natural hypertrophy usually ends at full growth.
Since testosterone is one of the body’s primary growth hormones, men typically have around 60% greater muscle mass than women and find hypertrophy to be considerably easier to accomplish (absolutely).
Increasing testosterone levels, like with anabolic steroids, will improve outcomes. It is also regarded as a performance-enhancing substance, and using it might result in participants’ suspensions or bans from contests.
In most nations, testosterone is also classified as a medicinally controlled medication, meaning that it is unlawful to possess without a prescription. Gynecomastia, cardiac arrest, and testicular shrinkage can all result from anabolic steroid usage.
In the long run, anabolism and therefore muscle growth benefit from a positive energy balance, which occurs when more calories are ingested than burnt.
Athletes exercising for muscular growth have elevated protein synthesis, which can be attributed to an increased protein need. But whether or not strength-trained athletes need more protein is a matter of debate among scientists.
Training factors like frequency, intensity, and total volume have a direct impact on the development of muscle hypertrophy in the context of strength training.
Muscular hypertrophy may be achieved by gradually increasing each of these training factors.
Changes in protein synthesis and muscle cell biology associated with stimuli
Protein synthesis
The message permeates down to change the gene expression pattern. The extra contractile proteins seem to be integrated into the existing myofibrils (a muscle cell’s chain of sarcomeres).
It seems that there is a maximum size at which a myofibril can grow before splitting. Every muscle fiber appears to be involved in these processes.
That is, rather than a rise in the total number of muscle cells, hypertrophy is predominantly caused by the expansion of individual muscle cells.
However, skeletal muscle cells are distinct from other body cells in that they can have numerous nuclei, and that number can rise.
Cortisol hinders protein synthesis and reduces the absorption of amino acids by muscular tissue.
In young males who are nourished appropriately, the brief boost in protein synthesis that follows resistance training returns to normal after around 28 hours.
A further study found that even 72 hours after exercising, there was an increase in muscle protein synthesis.
Eating 340 grams of lean beef did not result in any greater increase in muscle protein synthesis than eating 113 grams of lean beef, according to short research done on young and old. Protein production in the muscles rose by 50% in both groups.
According to the study, giving young and old people more than 30 g of protein in a single meal did not further stimulate their muscles’ protein production. The findings drawn from this research are debatable because the study needed to examine protein production in connection to training.
According to a 2018 analysis of the scientific literature, 1.6 g of protein per kilogram of body weight is necessary to develop lean muscle tissue. This amount of protein can be spread throughout the day over 4 meals or snacks.
Bodybuilders frequently recommend consuming 2-4 grams of protein per kilogram of body weight each day.
Though higher than necessary, according to scientific literature, protein intakes above 1.8 g per kilogram of body weight did not appear to have a bigger effect on muscle growth.
According to a 2002 American College of Sports Medicine research, athletes should consume 1.2–1.8 g of protein daily per kilogram of body weight.
On the other hand, Di Pasquale (2008) suggests a minimum protein intake of 2.2 g/kg “for anyone who participates in intense recreational or competitive sports and wants to maximize lean body mass without gaining weight.” Di Pasquale (2008) bases this recommendation on recent studies.
Microtrauma
Small injury to the muscle fibers is known as microtrauma. It’s still unclear exactly how microtrauma and muscle development relate to one another.[Reference required]
According to one notion, muscle development is significantly influenced by microtrauma.
The body overcompensates when microtrauma (from weight training or other hard activities) happens, creating new tissue to replace the injured one and lowering the likelihood of further injury.
Progressive overload is crucial to ongoing development because, as the body adjusts and grows more resilient to stress, damage to these fibers may be the root cause of delayed onset muscular soreness (DOMS) symptoms.
However, another research analyzing the temporal evolution of modifications in muscle protein synthesis and their connection to hypertrophy revealed that damage was not connected to hypertrophy.
The authors of one study demonstrated that protein production was not focused on muscle development until the injury had healed.
Myofibrillar vs. sarcoplasmic hypertrophy
Sarcoplasmic or myofibrillar hypertrophy are the two forms of skeletal muscle hypertrophy that are often identified in the bodybuilding and fitness world, as well as in educational literature.
This theory states that while myofibrillar hypertrophy results in an increase in the number of actin and myosin contractile proteins, which increase muscular strength and cause a slight increase in muscle size, sarcoplasmic hypertrophy causes an increase in the volume of sarcoplasmic fluid in the muscle cell but does not cause an increase in muscular strength.
Sarcoplasmic hypertrophy is more prevalent in bodybuilders’ muscles since research indicates that it demonstrates a larger increase in muscle size, but myofibrillar hypertrophy is more prevalent in Olympic weightlifters’ muscles and increases total physical strength.
In sports
Professional competitors with significant muscular hypertrophy can be seen in a variety of strength-related sports, including professional wrestling, boxing, mixed martial arts, Olympic weightlifting, rugby, and gymnastics.
To better fit their position of play, athletes in other more skill-based sports like football, ice hockey, baseball, basketball, and hockey may also train for improved muscular hypertrophy.
In basketball, for instance, a center may wish to bulk up and gain more muscle to better dominate opponents in the low post.
In addition to receiving intensive strength training, athletes preparing for these sports also receive substantial cardiovascular and muscular endurance training.
Pathology
An MRI or muscle biopsy can demonstrate that a skeletal muscle has indeed hypertrophied in one or more cases of neuromuscular disorders.
This muscular hypertrophy is referred to as having a pseudo-athletic look since it is not the consequence of resistance training or strenuous physical work.
Since muscle hypertrophy is a reaction to intense anaerobic exercise, diseases that cause premature muscle fatigue (neural or metabolic), interfere with the excitation-contraction coupling in muscle, or result in repeated or prolonged involuntary muscle contractions (fasciculations, myotonia, or spasticity) would make routine daily activities difficult.
Although the muscles in lipodystrophy are quantifiably hypertrophic, the aberrant loss of subcutaneous fat amplifies the look of the muscles.
Certain diseases, such as muscular dystrophies, metabolic myopathies, endocrine myopathies, congenital myopathies, non-dystrophic myotonias and pseudo myotonias, denervation, spasticity, and lipodystrophy, can cause genuine muscle hypertrophy.
Depending on the duration of the illness, the muscular hypertrophy may continue, fade thereafter, or develop into pseudohypertrophic muscle atrophy (muscle atrophy with infiltration of fat or other tissue).
For example, genuine muscle hypertrophy may initially occur in Duchenne and Becker muscular dystrophy, but eventually, pseudohypertrophy may emerge.
Diet and Muscle
Maintaining your fitness level requires eating a healthy, balanced diet. Intake of protein is particularly crucial for those who want to gain muscular growth.
According to current recommendations, male and female adults should consume 56 grams (g) and 46 grams (g) of protein daily, respectively.
The time of protein consumption can also be significant. Consuming 20 g of dietary protein during or right after exercise may help boost muscle protein synthesis, minimize protein breakdown, and promote more efficient muscle reconditioning, according to a 2013 Nestlé Nutrition Institute Workshop Series report.
Sources of protein include:
- beef
- lamb
- pork
- poultry
- fish
- eggs
- milk
- milk products, like cheese
Non-animal sources of protein include foods like:
- soybeans
- beans
- nuts
- seeds
Summary
Increasing muscle growth is known as muscular hypertrophy, and this is usually achieved by strength training.
Working exercise puts demand on the muscles, which prompts the body to repair and grow more muscle fibers.
Strength and muscle size increase with the number of muscular fibers in the muscle. Many exercises against resistance can be a part of strength training. Over time, increasing the resistance will cause the muscles to become larger.
It may take some time for muscular hypertrophy to result in appreciable gains in strength or size.
To maximize muscular growth and strength, people should combine strength training with healthy habits like eating a balanced diet and obtaining enough sleep.
FAQ
Loss of muscle mass is known as muscular atrophy. Your muscle mass will rise if you have muscular hypertrophy. The fibers in your muscles enlarge or thicken. Your muscle cells’ volume increases as a result of muscular hypertrophy.
The cause of physiological hypertrophy is a common stressor. For instance, skeletal muscle growth is brought on by exercise. A pathologic stressor is the cause of pathologic hypertrophy—for instance, an increase in heart size brought on by aortic stenosis.
The goal of muscle building is to cause muscle tissue to hypertrophy, increasing in overall muscular size. Strength training, on the other hand, tries to improve the muscles’ capacity for function. Higher training volume, more frequent sessions, and shorter rest intervals between sets are necessary for hypertrophy training.
Muscle hypertrophy generally indicates that your muscles are reacting to resistance training exercises or are expanding properly, which is a healthy thing. Hypertrophy can occasionally be dangerous, particularly in conditions affecting the heart muscle tissue.
Four Advantages of Hypertrophy Training
Strength: Training for specific muscle parts to hypertrophy can result in stronger, more weight-lifting muscles. 3. Reduce body fat: Training for muscle hypertrophy has the same fat-losing effects as a strength training regimen.
Studies show that the best stimulus for increasing muscle growth is to execute 15 to 20 sets of hard hypertrophy exercises per week. It is advisable to distribute the burden throughout the week because a particular exercise can only produce a maximum muscle reaction after 5–6 sets.
After exercise, protein is essential because it aids with muscle repair. McMahan advises consuming at least 20 grams of protein immediately after strenuous exercise. According to her, healthy sources include fish, poultry, eggs, and protein bars or shakes. Additions like chocolate milk are excellent.
One to three minutes of rest
Resting for one minute in between sets of eight to twelve repetitions is the conventional wisdom for optimizing muscle growth, or hypertrophy. However, a new study indicates that the real sweet spot maybe three minutes.
Phase of Hypertrophy (2–6 Months) After training each muscle group, if any, you won’t experience as much pain or ache as you did throughout the adaptation phase. Greetings from Volume Prepare to lift more weight, perform fewer repetitions, and take fewer breaks.
It turns out that including exercise in your session will help you get the most out of it. A separate 2021 study supports the findings of a 2015 study that says warming up with aerobic exercise before working out with weights can promote protein metabolism and muscle growth.

7 Comments