Humerus Bone
Table of Contents
Introduction of the humerus bone
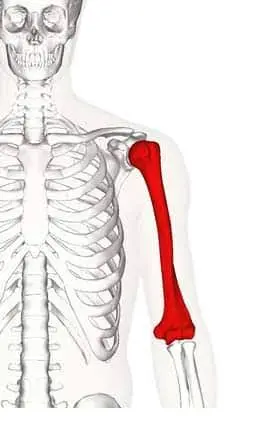
The humerus is a long bone located in the upper arm or forelimb of vertebrates, extending from the shoulder to the elbow.
Defines the human brachium, or arm. It articulates distally at the elbow joint with the radius and ulna, and proximally with the glenoid through the glenohumeral (GH) joint. The head of the humerus, which creates a ball and socket joint with the glenoid cavity on the scapula, is the most proximal part of the humerus.
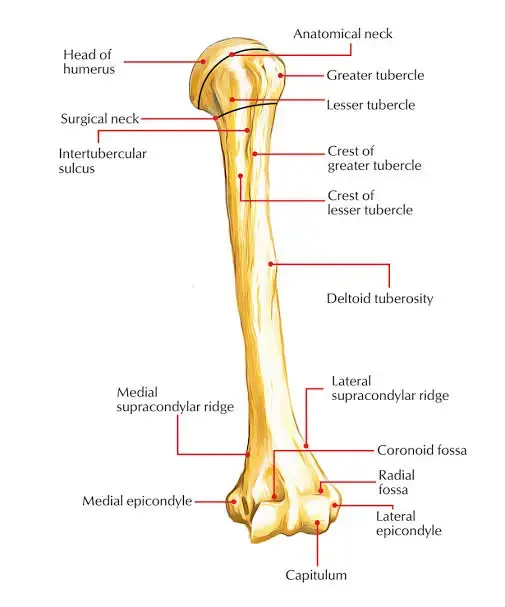
The anatomical neck of the humerus, which separates the humeral head from the greater and lesser tubercles, is located directly beneath the humeral head. The remaining epiphyseal plate makes up the humerus’ anatomical neck. The two tubercles are distinguished vertically by an intertubercular groove that is visible proximally. The humeral surgical neck comes after the tubercles which have clinical significance in case of fracture.
The humerus’s cylindrical shaft continues distally, with a radial groove (also known as the spiral groove) on its posterior aspect and a deltoid tubercle on its lateral aspect The bone that makes up the medial and lateral epicondyles widens at the distal end of the humerus. The trochlea, capitulum, olecranon, coronoid, and radial fossae make up the condyle, which is where the distal portion of the humerus ends.
The lateral capitalism, which articulates with the radius bone head, is located on the anterior lateral surface of the condyle, while the trochlea, located on the anterior medial surface of the condyle, articulates with the trochlear notch of the ulna bone.
The radial fossa, which receives the head of the radius upon flexion of the elbow joint, is situated on the anterior surface of the condyle, superior to the capitulum and accommodating the coronoid process of the ulna. This is known as the coronoid fossa, which is situated superior to the trochlea. The olecranon fossa, located on the posterior surface of the condyle, articulates with the olecranon of the ulnar bone when the elbow joint flexes.
Structure of the Humerus Bone
The glenohumeral joint is a synovial ball and socket joint formed by the articulation of the humeral head with the glenoid fossa of the scapula. The activation of the rotator cuff muscles (teres minor, subscapularis, supraspinatus, infraspinatus, pectorals major, and deltoid) determines the range of motion in this joint, which includes internal and external rotation, abduction and adduction, flexion, and extension.
The glenohumeral joint is home to several synovial bursae, such as the subacromial, sub-deltoid, sub-coracoid, and coracobrachialis bursa, which facilitate frictionless movement. The GH joint is stabilized by the coracoacromial and acromioclavicular ligaments, which also stop the humerus from migrating proximally. The elbow joint, a synovial hinge joint, is formed by the articulation of the capitulum and trochlea of the humerus with the head of the radius bone and trochlear notch of the ulna.
The complexes of the radial (lateral) and ulnar (medial) collateral ligaments stabilize this joint. Three parts make up the ulnar collateral ligament (UCL):
The strongest and most important stabilizer against valgus stress forces is the anterior oblique band.
runs from the humerus’s medial epicondyle to the proximal ulna’s sublime tubercle.
The posterior component of the UCL exhibits the largest change in tension from flexion to extension range of motion (ROM) at the elbow. Posterior oblique band: tightest in flexion.
The transverse ligament adds very little, if anything, to the stability of the elbow joint. Here, too, an olecranon bursa helps to lessen friction during motion. The muscles of the biceps brachia, coracobrachialis, and triceps are primarily responsible for elbow movement. It should be noted that in anatomical position, the antebrachial and humerus form a carrying angle rather than perfectly aligning. This angle can range from 5 to 10 degrees in males and up to 18 degrees in females. An excessive lateral deviation is called cubits valgus, and an excessive medial deviation is called cubitus varus. This angle permits the hips to be cleared.
Embryology of the Humerus Bone
The humerus is a long bone that grows through endochondral ossification, one of the many long bones in the appendicular skeleton. The replacement of a cartilage template with bone characterizes this process.
Mesenchymal cells that form cartilage-secreting chondrocytes first lay down a comparatively small model of cartilage. Second, chondrocyte hypertrophy and the secretion of factors like alkaline phosphatase to encourage calcification of that cartilage are present in the ossification centre, the centre of the cartilage template.
This results in a nutrient blockage and chondrocyte death. But these cells also secrete vascular endothelial growth factor (VEGF) to promote angiogenesis within the calcifying cartilage before dying. The Indian hedgehog homolog (IHH) protein, in the meantime, causes cells outside of the perichondrium to differentiate into blasts.
and create the bony collar, a layer of bone that encircles the cartilage’s centre.
With time, a core region of dead chondrocytes forms, surrounded by a shell of bone, small remnants of calcified cartilage, and a vascular supply encircling the interior. Internal mesenchymal cells that differentiate into more osteoblasts and monocytes that form osteoclasts are brought in by the vascular supply.
Bone is resorbed on the inside and deposited on the outside in the centre of the original cartilage template, causing the hollow entity (forming a marrow) to widen. Concurrently, as secondary ossification centres, chondrocytes are continuing to proliferate at the proximal and distal ends of the cartilage template.
This process permits cartilage to grow at the bones, offering capacity for vertical expansion. In the end, the linear zone of cartilage known as the epiphyseal plate is formed by the junction of bone and cartilage. Here, cartilage replaces bone continuously until bone growth fully fuses and ceases at puberty. There are eight distinct ossification centres in the humerus: the humeral shaft, the medial and lateral epicondyles, the olecranon, the greater and lesser tubercles, and the head of the humerus.
The ossification of the shaft happens at eight weeks of gestation, while the ossification of the humeral head happens either at birth or shortly after. In the first year of life, the greater tubercle ossifies, and in the first six years of life, the lesser tubercle ossifies. All of the humerus’s proximal ossification centres have completely fused with the osseous structure by the time an adolescent
Humerus bone in the other animals
The limbs of early amphibian fossils were extremely short because they had little or no shaft connecting their upper and lower extremities. However, the humerus shares a human-like shape with the majority of extant tetrapods.
The lower extremities of many reptiles and certain mammals (when they are in the primitive state) have a sizable aperture called the entepicondylar foramen that allows blood vessels and nerves to flow through.
Blood supply of the humerus bone
The anterior and posterior circumflex humeral arteries anastomose provide the proximal humerus with its main blood supply. The distal third of the axillary artery gives rise to these branches. The posterior humeral circumflex artery may be the main blood supply source for the humeral head, according to recent research. The arcuate artery, which supplies most of the greater tuberosity, is the terminal division of the anterior humeral circumflex artery.
The axillary artery continues to develop into the brachial artery, which will supply blood to the rest of the humerus and the muscles attached to it, along with the refund brachia artery, one of its branches. Nutrient arteries supply blood flow to the interior regions of the humerus, branching off from the brachial artery.
Nerve supply of the Humerus Bone
The axillary nerve is produced from the posterior cord of the brachial and wraps around the surgical neck of the humerus. Specifically, the musculocutaneous nerve, which arises as a division of the brachial plexus’s lateral cord, supplies the teres minor Innervation of the front region of the brachium.
The lateral cutaneous nerve of the forearm is where this nerve ends after passing through the coracobrachialis muscle and between the biceps brachii and coracobrachialis. The brachial artery, the long head of the triceps, the spiral groove of the humerus, and the posterior cord of the brachial plexus are all crossed by the radial nerve. It provides innervation to the forearm, surrounding skin, and posterior arm muscles.
The radial nerve is also responsible for the innervation of the lateral and medial epicondyle of the humerus One should note that the median nerve and ulnar nerve likewise come off the brachial plexus and travel down along the brachium, however, do not supply innervation to this region of the forearm, arm, and skin that is on top. The lateral and medial epicondyles of the humerus are innervated by the radial nerve as well. It should be noted that although the ulnar and median nerves also emerge from the brachial plexus and descend the brachium, they do not provide innervation to this area.
What is the location of the Humerus?
The only bone in your upper arm is the humerus. It extends from your elbow to your shoulder.
What is the function of the Humerus?
Your humerus performs numerous vital functions, such as:
The upper limb’s ability to move, particularly the arm, is greatly dependent on the humerus bone. To move the arm and shoulder joints, it acts as an attachment point for several muscles, tendons, and ligaments. The humerus bone serves many important purposes, including
Shoulder joint movement: A variety of shoulder movements, including abduction, adduction, flexion, extension, and rotation, are possible because the humerus bone and the scapula bone form a ball and socket joint.
Attachment of muscles The muscles that move the arm and shoulder joint attach to the humerus bone’s numerous bony projections, ridges, and depressions. Attachment sites are provided by the greater and lesser tubercles on the proximal end. Weight-bearing: To maintain a stable arm and shoulder joint, the humerus bone helps transfer the weight of the upper limb to the rest of the body.
Production of blood cells Red and white blood cells, which are essential for immune system performance and the body’s ability to carry oxygen, are produced in the bone marrow found inside the humerus bone.
The main purpose of the humerus bone is to provide attachment points for muscles, tendons, and ligaments, which permits movement of the arm and shoulder. It is a crucial bone for proper body function since it aids in blood cell production and weight bearing.
What is the humerus’s size?
Your humerus is the largest bone in your body, excluding the bones in your legs. The humerus bones of most adults are about one foot long.
Region of the Humerus bone
The upper end of the humerus bone
The greater and lesser tuberosity, the intertubercular sulcus, the anatomical neck, and the surgical neck all identify the proximal humerus.
The head is located at the upper end of the humerus. The anatomical neck divides this from the greater and lesser tuberosity and it faces medially, upward, and backward.
There are anterior and posterior surfaces to the larger tuberosity, which is situated laterally on the humerus. Three rotator cuff muscles attach to the greater tuberosity at this location: the supraspinatus, infraspinatus, and teres minor. These muscles attach to the superior, middle, and inferior facets, respectively.
The smaller and more medially positioned lesser tuberosity is situated on the bone. There is just the anterior surface. It serves as the point of attachment for the subscapularis, the final rotator cuff muscle. The intertubercular sulcus is a deep groove that divides the two tuberosa. This groove is where the tendon of the long head of the Biceps Brachii Muscle emerges from the shoulder joint.
Lips are the boundaries of the intertubercular sulcus. Intertubercular sulcus lips are where the latissimus dorsi, pectorals major, and teres major insert. The phrase “a lady between two majors” can help you recall this, as the latissimus dorsi attaches laterally to the pectorals major and medially to the teres major on the medial lip.
The surgical neck reaches the humeral shaft immediately distal to the tuberosity’s. Here, the circumflex humeral vessels and the axillary nerve are pressed up against the bone.
The shaft of humerus bone
Several muscles attach to the humeral shaft. It is flattened distally and circular proximally, according to cross-section views.
The deltoid muscle attaches to a roughened surface on the lateral side of the humeral shaft. The deltoid tuberosity is the name given to this.
A shallow depression parallel to the deltoid tuberosity that runs diagonally down the posterior surface of the humerus is known as the radial (or spiral) groove. This groove is home to the prefund brachia artery and the radial nerve. Along the shaft of the humerus, the following muscles attach: Coracobrachialis, deltoid, brachialis, and brachioradialis are the anterior muscles.
The spiral groove marks the origins of the medial and lateral heads of the triceps located posteriorly.
The distal end of the humerus bone
Medial and lateral supracondylar ridges are formed by the lateral and medial borders of the distal humerus. The site of the common origin of the forearm extensor muscles is the more rugged lateral supracondylar ridge.
The lateral and medial epicondyles are extra scapular bone projections located directly distal to the supracondylar ridges. You can feel both at the elbow. Out of the two, the medial is larger and extends farther away. There is a palpable groove on the posterior aspect of the medial epicondyle where the ulnar nerve passes.
The trochlea distally is situated medially and extends onto the bone’s posterior aspect. The capitulum articulates with the radius lateral to the trochlea. Additionally situated on the humerus’ distal end are three coronoid, olecranon, and radial fossa.
Articulations of the humerus bone
The glenohumeral joint, also known as the shoulder joint, is formed when the proximal region of the humerus articulates with the glenoid fossa of the scapula.
The trochlea of the humerus articulates with the trochlear notch of the ulna, and the capitulum of the humerus articulates with the head of the radius at the elbow joint.
Muscle attachment in the Humerus bone
Numerous muscles of the upper limb, which are classified as scapulohumeral, anterior compartment, and posterior compartment muscles, originate and insertion point on the humerus.
Scapulohumeral muscles: The acromion of the scapula, the scapula’s spine, and the clavicle are the three points of origin of the deltoid muscle, which defines the upper limb’s shoulder contour. Each of these parts inserts into the humerus’s deltoid tuberosity. The deltoid muscle permits humeral abduction and adduction as well as internal and external rotation.
The clavicle, manubrium, sternum body, and true ribs are the points of origin of the pectorals major muscle, which inserts into the humerus’s intertubercular sulcus. It permits the humerus to adduction, flexion, extension, and medial rotation.
The rotator cuff is made up of four muscles: the infraspinatus, supraspinatus, subscapularis, and teres minor, To enable internal rotation of the humerus, the subscapularis muscle attaches itself to the lesser tubercle of the humerus after emerging from the subscapular fossa of the scapula. To enable humeral abduction, the supraspinatus muscle inserts into the greater tubercle of the humerus after starting in the supraspinous fossa of the scapula.
The greater tubercle of the humerus is where the infraspinatus muscle inserts after emerging from the scapula spine and infraspinatus fossa. This muscle permits the humerus to rotate externally. Internal rotation and adduction are made possible by the teres major, which inserts into the lesser tuberosity of the humerus from the inferior angle of the scapula. The teres minor inserts into the greater tubercle after beginning on the lateral border of the scapula, enabling external rotation.
Anterior compartment muscles: The biceps brachia muscle does not have an actual origin or insertion site on the humerus, but it does have a long and short head. But the tendon of the biceps brachia long head passes through the transverse humeral ligament, which extends from the lesser tubercle to the greater tubercle of the humerus and changes the humeral intertubercular groove into a canal.
This tendon originates on the supraglenoid tubercle of the scapula and ends at the radius. The scapula’s coracoid process is the starting point of the coracobrachialis, which inserts onto the humerus’ medial surface to permit flexion and internal rotation. Originating on the anterior surface of the distal humerus, the brachialis muscle inserts onto the ulna forearm.
Muscles of the posterior compartment: The triceps brachia muscle has three heads: the lateral head originating on the posterior surface and the medial head originating on the posterior aspect of the humerus, inferior to the spiral groove.
Both heads insert into the olecranon process of the ulna, enabling forearm extension at the elbow joint. Notably, the posterior circumflex artery, vein, and radian nerve passes through a quadrangular space formed by the humerus, the long head of the triceps, and the teres major and teres minor.
Clinical Pathology of the Humerus Bone
Clinical pathology of the humerus bone is mentioned below, Let check the different pathological conditions related to the humerus.
Typical Trauma to the Humerus Bone, Although the humerus bone is robust, overuse or trauma can still cause injuries. The following are typical humerus bone injuries:
Fractures of the Humerus
Fractures of the humerus are frequent, particularly in elderly individuals. Although fractures can happen anywhere on the bone, they most frequently happen at the proximal end, close to the shoulder joint. Overuse, falls, and direct impact are all potential causes of fractures.
Dislocations
The most frequent kind of humerus bone dislocation is a shoulder dislocation. A fall or direct impact can cause the humerus bone to dislocate from the shoulder joint, resulting in pain, swelling, and restricted movement.
Injuries to the rotator cuff
The rotator cuff is a collection of muscles and tendons that support and stabilise the shoulder joint by attaching to the humerus bone. Overuse, repetitive motions, or trauma can result in rotator cuff injuries, which can cause pain, weakness, and restricted movement.
Bursitis
Bursa are tiny sacs filled with fluid that cushion joints and lessen friction between soft tissues and bones. Bursitis is caused by bursa. Pain and swelling can result from bursa inflammation near the shoulder joint, which can be brought on by overuse, repetitive motions, or direct trauma.
Tendinitis
Pain, stiffness, and restricted mobility are caused by inflammation of the tendons that attach to the humerus bone. Overuse or repetitive motions, like lifting weights or tossing a ball, can result in tendinitis.
Damage to the Radial Nerve
After a humeral fracture, one of the most frequent peripheral nerve injuries is radial nerve palsy. Unless nerve recovery (as shown in EMG/NCS studies) does not occur within 3 to 6 months, treatment usually consists of observation. Proponents of early radial nerve exploration point to substantial internal patient function loss and delayed repair as reasons against delayed exploration. Radial nerve damage can result from trauma or fracture at the mid-shaft or radial groove.
Condition of the Shoulder
Adhesive capsulitis of the shoulder (also known as frozen shoulder syndrome) and calcific tendinitis of the rotator cuff are two relatively common conditions with debatable and/or complex aetiologies. Exercise and rest are the main forms of treatment; surgery is rarely necessary. However, treating frozen shoulder syndrome surgically infiltration under general anaesthesia.
Osteoporosis
Usually, there aren’t any overt signs.
Osteoporosis is more common in women or those classified as female at birth (AFAB) and in adults over 50. See your doctor about a bone density test, which can identify osteoporosis early on and prevent fractures.
Metastatic bone disease
Destructive bone lesions and severe localized pain are symptoms of metastatic bone disease, which typically affects the humerus. The chance of a humeral fracture can be raised by lesions. External beam irradiation is used as a form of treatment for patients whose lesions do not cover 50% of the cortex.
Nevertheless, with destructive lesions affecting over 50% of the External beam irradiation is the treatment of choice for patients whose lesions do not occupy more than 50% of the cortex. However, intramedullary nailing combined with postoperative external beam radiation is the treatment of choice for destructive lesions involving more than half of the cortex. If the disease worsens, bone resection or reconstruction may be necessary.
Miscellaneous condition
Humerus varus can be brought on by hematologic, infectious, genetic, or neurological conditions. The lateral part of the proximal humerus will grow more quickly in this situation, while the medial portion will not develop properly. This disorder results in a varus rotation of the humerus, which limits flexion at the shoulder joint and reduces arm abduction. Functional impairment is uncommon, though. Using a plate screw fixation, a valgus osteotomy of the humerus is the surgical procedure.
A rare musculoskeletal disorder known as disappearing bone disease is characterised by bone resorption, insufficient bone formation, and insufficient vascular proliferation. This illness has serious consequences for one’s quality of life. Similar to this, resorption of the osseous matrix combined with a lack of bone formation characterises Gorham-Stout disease in the humerus. Although the cause of the condition is unknown, there is a lymph vascular malformation in the bone. Aching pain, deteriorating weakness, and subsequent fractures are common symptoms. Treatment is difficult and consists of a mix of radiotherapy, medication, and surgery.
A rare condition called Charcot arthroplasty is characterized by crippling joint destruction. In addition to changing muscular control, the disease may cause bone and soft tissue loss around the humerus. An arthroplasty of the shoulder is the treatment. Osteochondritis dissecans and Panner disease are linked to humeral Osteochondritis. The two illnesses manifest comparably. Avascular necrosis of the capitulum is the hallmark of Panner disease, which usually manifests between the ages of 7 and 10, earlier than that of Osteochondritis dissecans. Generally speaking, surgery is not used to treat panner disease
Diagnosis of humerus pathologic conditions
A bone density test is the most often performed procedure to evaluate the condition of your humerus. It is also referred to as a DXA or DEXA scan. A bone density test uses low doses of X-rays to gauge how strong your bones are. It serves as a gauge for bone loss with ageing.
Your surgeon or healthcare provider may require imaging tests if you have had a humeral fracture. These tests may include:
- radiography. Also known as X-ray,
- Imaging with magnetic resonance (MRI).
- CT scan.
Treatment of the humerus pathologic conditions
Treatment for your humerus is typically not necessary unless you have had an arm injury, such as a fracture. If osteoporosis is diagnosed, treatment may be necessary.
Treatment for humerus fractures
The cause of your fracture and the location of the break in your humerus will determine how it is treated. You’ll require immobilization in the form of a cast or splint, and surgery may be necessary to realign (set) your bone in its proper position and keep it there so that it can heal.
Treatment for osteoporosis
Osteoporosis can be treated with medication, exercise, and vitamin and mineral supplements.
To prevent osteoporosis, you usually only need to exercise and take supplements.
Treatment for shoulder dislocation and rotator cuff
Rotator cuff injuries and shoulder dislocations will be diagnosed and treated by a medical professional. The majority of persons who suffer a dislocated shoulder must wear a sling for weeks.
Surgical significance in humerus bone pathologic conditions
Proximal humeral fractures can occur in elderly patients who fall on their shoulders or on their outstretched arms. Shoulder pain and limb immobility are the symptoms of this injury. In addition to causing long-term morbidity, multiple fragmentations of these proximal fractures may also result in post-traumatic osteonecrosis.
Treatment for most proximal humerus fractures is non-operative. However, because they have less bone remodelling and growth, elderly patients with severe displacement can benefit from surgical intervention. Interventional options include intramedullary nailing, cannulated screws, threaded wires, and smooth wires for internal fixation. For glenohumeral dislocations, rotator cuff tears, joint disease, and proximal humerus fractures in the elderly, reverse shoulder arthroplasty is an additional option. Inflammatory arthritis and shoulder osteoarthritis may also be indications for shoulder arthroplasty.
Young, active patients frequently experience anterior glenohumeral dislocation.38 Displacement fractures involving the greater tuberosity of the humerus can impinge on the subacromial impingement and the rotator cuff muscles. When displacements exceed 3 mm, surgery is typically necessary.
After a fall or other trauma, children three years old and younger may suffer transphyseal fractures of the distal humerus. The cubitus varus will be visible on radiologic imaging, and the humerus and forearm bone will not align with the standard carrying angle. Techniques for percutaneous pinning and closed reduction should be used during surgery. Growth arrest and condyle osteonecrosis are frequent aftereffects. Surgical intervention typically consists of dome, multi-planar, or lateral closing wedge osteotomies.
Surgery is frequently used to treat distal humerus intercondylar fractures using an olecranon osteotomy. Avascular necrosis can result from post-traumatic supracondylar humeral fractures because the trochlear blood supply is cut off. Patients may not show any symptoms at the time of the injury, but within six months necrosis-related pain or movement loss may occur.
How to keep the humerus bone healthy?
You can keep your bone (and overall) health in check by maintaining a healthy diet and exercise routine as well as by visiting your doctor for routine examinations. Ask your doctor about a bone density scan if you are over 50 or if osteoporosis runs in your family.
Follow these general safety tips to reduce your risk of injury:
- Wear your seatbelt at all times.
- Ensure that nothing could trip you or others in your home or workspace.
- When reaching for objects at home, always use the appropriate tools or equipment. Never stand on countertops, tables, or chairs.
- Employ a walker or cane.
Quick information regarding the Humerus Bone
- The humerus is a lengthy bone. The femur in your upper thigh and the radius and ulna in your forearm are examples of additional long bone types.
- To length, the humerus is the longest bone in your arm
- You are not striking your humerus when you strike your “funny bone,” despite its moniker. The ulnar nerve, which is situated behind your elbow joint, is what you’re striking.
- Your hands and arms have a higher risk of breaking bones. This is because humans frequently employ these body parts to break falls or lessen the force of blows or traumas.
Summary
The humerus is the name of the upper arm bone. Except for the bones in your leg, it is the longest bone in your body. It’s necessary for the range of motion in your arm. Your humerus also supports many essential muscles, ligaments, tendons, and parts of your circulatory system.
To help you regain your strength and range of motion, physical therapy may also be necessary in addition to surgery to repair your humerus. Osteoporosis can affect any bone, including the humerus. Your humerus is connected to a vast network of muscles and nerves, so injuries to one can often affect the others.
An essential component of the human skeleton that permits arm movement is the humerus bone. Its three sections—the shaft, the distal end, and the proximal end—each have unique structures that support their respective functions. A variety of arm movements are made possible by the humerus bone in cooperation with the upper limb muscles.
A humerus bone injury can seriously impair arm function and necessitate immediate medical attention. The course of treatment for injuries to the humerus bone varies according to the severity of the injury and can include surgery as well as conservative measures like rest, ice, and pain medication.
In general, the significance of the humerus bone cannot be emphasized because the body must function properly.
FAQs
Humerus comprises latissimus dorsi, deltoid, and rotator cuff muscles, which move the arm, pectorals major
The anatomy of your upper arm muscles includes:
Brachii biceps. The brachialis is the muscle in the middle of your upper arm that makes up your biceps. It’s the deep muscle under your biceps.
The coracobrachialis. This muscle joins to your scapula, or shoulder blade, just beneath your biceps.
The biggest bone in the upper extremities, the humerus defines the human brachium, or arm.
Long bones in the upper extremities of the body.
References
- Rohit, B. (2023, April 17). Humerus bone – Anatomy, location, function – Samarpan Physio. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/humerus-bone/.
- Wikipedia contributors. (2023c, November 26). Humerus. Wikipedia. https://en.m.wikipedia.org/wiki/Humerus
- Volker, J. H. (2021, November 2). Humerus Bone Anatomy – Earth’s Lab. Earth’s Lab. https://www.earthslab.com/anatomy/humerus/https://www.earthslab.com/anatomy/humerus/
- Mostafa, E. (2023, August 7). Anatomy, shoulder and upper limb, humerus. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK534821/
- Professional, C. C. M. (n.d.-j). Humerus. Cleveland Clinic. https://my.clevelandclinic.org/health/body/24612-humerus
- Seladi-Schulman, J., PhD. (2022, February 28). The humerus bone: anatomy, breaks, and function. Healthline. https://www.healthline.com/health/humerus-bone#fast-facts
- MBChB, C. O. B. (2023, October 30). Humerus. Kenhub. https://www.kenhub.com/en/library/anatomy/the-humerus
- TeachMeAnatomy. (2021, June 3). The humerus – proximal – shaft – distal – TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/bones/humerus/