Orbicularis Oris Muscle
Table of Contents
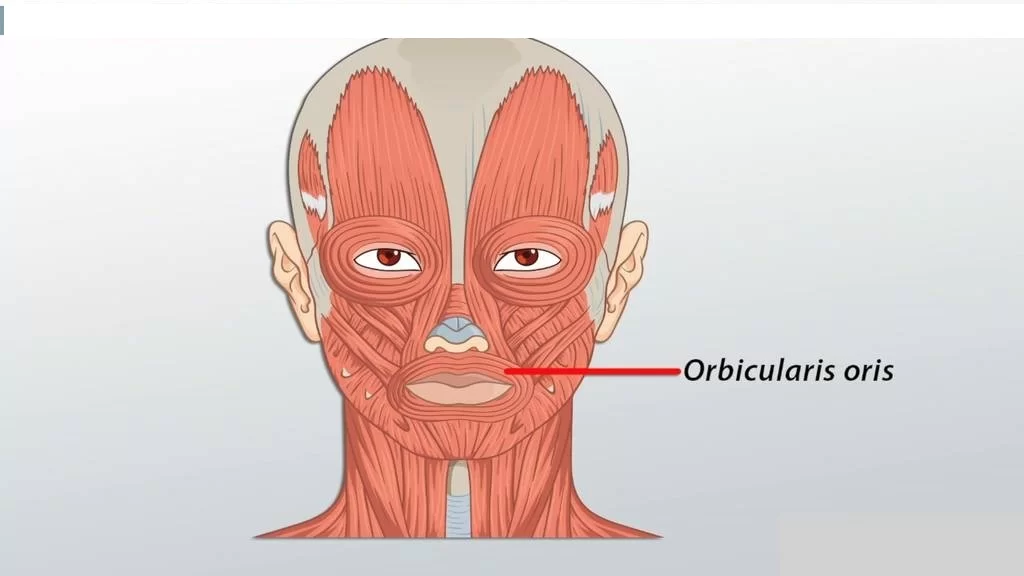
Orbicularis Oris Muscle Anatomy
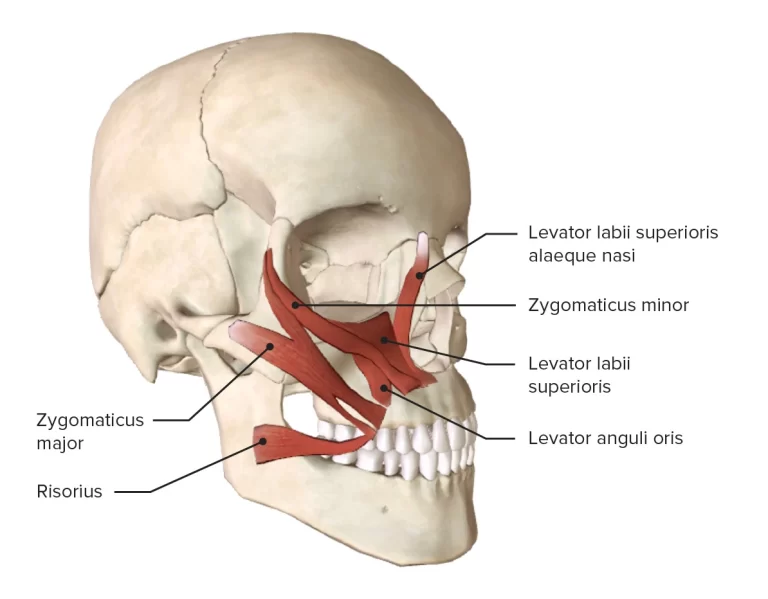
Orbicularis oris muscle is a complex and multi-layered muscle that attaches through a thin, superficial musculo-aponeurotic system to the dermis of the upper lip and lower lip and serves as an attachment site for many other facial muscles around the oral region.
Origin
It originates from the superior incisivus from the maxilla, and the inferior incisivus, from the mandible it is the thickest middle stratum, derived from the buccinator, thick superficial stratum, derived from elevators and depressor of lips and their angles.
Insertion
It inserts on the lips and angle of the mouth.
Nerve supply
The buccal branch of the facial nerve(CN VII) supplies the muscle.
Blood supply
The orbicularis oris is supplied with arterial blood mainly by the superior and inferior labial branches of the facial artery, the mental and infraorbital branches of the maxillary artery, and the transverse facial branch of the superficial temporal artery.
Muscle action

The orbicularis oris muscle helps in the opening and closing of lips and also helps in puckering of the mouth.
The orbicularis muscle has two purposes. The deep fiber causes the mouth’s sphincteric activity by acting as a constrictor. The “archaic” portion of the muscle is associated to retaining food due to general sphincteric activity as well as other muscular loops of the oropharynx. The superficial fiber, also known as the retractor fiber, is involved in speech modulation and precise lip motions.
Orbicularis oris pressurizes the dental arches and works in conjunction with the cheek muscles to produce speaking sounds by bringing the teeth and lips into contact. Additionally, swallowing, mastication, and sucking depend on it.
Because it aids in puckering the lips, this muscle is commonly referred to as the “kissing muscle.” When playing brass or wind instruments, the players use this muscle.
Previously, several authors expressed the belief that this muscle is a sphincter muscle since it surrounds the mouth’s aperture. The theory, however, was disproved by research showing that the muscle’s fibers actually move in a variety of directions rather than consistently in a circular motion.
Embryology
The muscle is a descendant of the second branchial arch’s mesoderm. Mesoderm of the second arch begins to thicken between the third and eighth weeks. Premyloblasts and myeloblasts, which initially form a sheet-like collection, start to stretch between 6 and 8 weeks to create five distinct laminae.
The mandibular lamina, which partially divides into the lower fibers of the muscle, and the infraorbital lamina, which develops into the higher fibers of the muscle, are the two embryonic laminae from which the orbicularis oris muscle is derived.
Physiologic Variantions
Some neonates may lack the orbicularis oris after birth, which causes a partial droop on the side of the face that is affected.
Strengthening exercise
- Using your index fingers, hook the corners of your mouth and gently pull towards the sides.
- Don’t overdo the stretch.
- Hold this position for a few seconds. Now work on the opposite side.
- Draw the corners of your mouth toward each other, resisting the movement using your index fingers again.
- Relax and repeat the exercise 25 times.
- The Orbiculais Oris muscle supports the overlaying skin and prevents sagging.
Related pathology
In facial palsy: The seventh cranial nerve, which supplies the muscle with nerves, can be injured and cause paralysis of the muscle. Drooling is caused by the orbicularis oris drooping in Bell palsy.
Tone loss: This muscle regulates the oral sphincter, which can contribute to drooling and trouble eating. Tone loss in this muscle causes the commissure to droop.
The orbicularis oris muscle, because of the orientation of its fibers, positively affects the stability of the denture, which has clinical implications for prosthodontics. In complete denture situations, the placement of the artificial teeth should be prioritized in order to prevent interference with muscle function and to facilitate the retention and stability action of the musculature.
The peri-oral muscles, particularly the buccinator and orbicularis oris, produce inward forces in the mouth cavity. The tongue’s outer forces counterbalance these forces. Muscle activity must be used to shape the impression for a complete denture so that it is harmonious with the nearby structures.
The tone of the orbicularis oris, the primary muscle of the lip, is influenced by the position of the teeth as well as the labial flange, which is located in the labial vestibule and extends from one side’s buccal frenum in the canine region to the other. As a result, this muscle affects the flange’s thickness.
The muscle is stretched when the mouth is opened widely, which narrows the sulcus. The denture will be displaced if the flanges are thick.
The orbicularis oris is strained if the teeth are positioned too labially. The stretching action of the lips against the teeth also has a tendency to push the maxillary denture out of place.
The buccinator mechanism, which consists of the orbicularis oris muscle, the buccinator, and the pharyngeal constrictor, plays a crucial part in the orofacial functions of swallowing, sucking, whistling, chewing, vowel pronouncing, and kissing. Food tends to collect in the oral vestibule during chewing if the buccinator and orbicularis oris muscles are weak or paralyzed.
Orbicularis Oris reflex (Snout reflex)
Infants’ top lips or lateral aspects of their noses can be tapped, which elevates the oral commissure on the ipsilateral side. Orbicularis oris reflex, often known as the snout reflex, is the name of this action. Later in life, this response naturally disappears.