
Quadratus Lumborum Muscle
Table of Contents
Quadratus Lumborum Muscle Anatomy
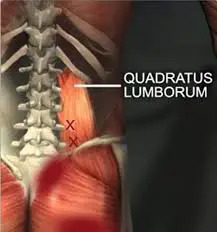
The iliac crest, the transverse processes of the lumbar vertebrae, and the 12th rib are all involved in the quadratus lumborum (QL), a muscle that is found in the deep and posterior, lateral, and inferior regions of the spine. Because of the complexity of the muscle structure, it might be challenging to pinpoint the exact functions that are achieved by fiber contraction.
It is an essential component of the fascia thoracolumbar. The fundamental cause of back pain may or may not be an aberration of QL, but this remains uncertain. The QL may serve as a junction point for the forces applied by nearby muscles, affecting the directions of the various tensions generated.
Because of its advantageous location and the entropic arrangement of its fibers, QL is a crucial access point for anesthesia when doing surgery on the abdomen, lower limbs, or back.
Structure
The thoracolumbar fascia, a myofascial system that covers the posterior region of the human body and includes a portion of the upper and lower limbs, includes the quadratus lumborum (QL) muscle as a fundamental component. The quadrangular-shaped and flattened QL muscle works in opposition to the abdominal muscles, generating an antagonistic force with the multifidus and erector spinae muscles.
The iliac crest, or inner lip, and the iliolumbar ligament supply the origin of the quadratus lumborum muscle, which is involved in the interior surface of the 12th rib and the transverse processes of the lumbar bodies of L1–L4.
Quadratus Lumborum Muscle Layers
Three layers make up QL, and each layer’s muscle fibers have a unique vector.
The superficial layer is a thin layer made up of muscle fibers with tendinous or even muscular terminations, known as iliocostal (from the iliac crest to the ribs) and iliothoracic (from the iliac crest to the lateral area of the vertebral body of T12).
Lumbocostal muscle fibers, which extend from the transverse processes of the lumbar vertebrae to the 12th rib, make up the intermediate layer. These are muscle fibers with a wide range of thickness, direction, and size.
Lateral iliocostal fibers and medially located iliolumbar fibers—which originate in the iliac crest and connect to the lumbar vertebrae’s transverse processes—make up the posterior layer. The thoracolumbar fascia may be involved by the iliocostal muscle bundles, which insert themselves with their tendon ends. In the caudal region, this layer is thicker, while in the rostral region, it is more tapered.
The very varied arrangement of QL muscle fibers makes it impossible to identify an exact pattern of orientation.
The transverse abdominal muscle’s aponeurosis is usually medially to the QL muscle.
Origin
Iliolumbar ligament and internal lip of Posterior iliac Crest.
Insertion
The medial half of the lower border of the 12th rib and tips of transverse processes of lumbar vertebrae.
Nerve Supply
The twelfth thoracic and first through fourth ventral rami of lumbar nerves (T12, L1-L4).
- Subcostal nerve (T12).
- Iliohypogastric and Ilioinguinal nerve (both from L1).
- Branches from the ventral rami (L2 and L3).
Blood Supply
The lumbar arteries and a lumbar branch of the iliolumbar artery provide QL with its circulatory supplies. The posterior face of the aorta, at the level of the first four lumbar vertebrae, gives birth to four lumbar arteries on each side. They eventually meet the QL muscle by running posteriorly behind the sympathetic chain and beneath the iliopsoas muscle’s arches tendon. The quadratus lumborum receives blood from the first three arteries posteriorly and the fourth anteriorly.
The internal iliac artery’s (also known as the hypogastric artery) first tributary is the iliolumbar artery. It rises beneath the iliacus muscle (iliac fossa), which receives its separate branches’ nourishment from the iliac muscle, and the psoas muscle. Its branches go into the transverse muscle of the abdomen, the QL, the psoas muscle, and a branch of the spinal canal that runs between the sacrum and the fifth lumbar vertebra.
Longitudinal anastomotic vessels connect the lumbar veins on either side, forming the ascending lumbar vein, a tiny vertical trunk. This vessel forms an important anastomotic pathway between the inferior vena cava system and the superior vena cava system. At the inferior end, it communicates with the iliolumbar vein and occasionally with the common iliac vein. At the superior aspect, it gives rise to the right azygos vein and the left hemizygous vein.
The inferior vena cava and the abdominal aorta are connected to the lumbar lymph nodes of the abdominal cavity, which drain the lymph from the QL.
Actions
maintain frontal plane stability of the pelvis.


Alone(unilateral), lateral flexion of the vertebral column; Together (bilateral), depression of thoracic rib cage.
Relations
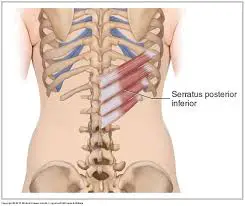
Because the quadratus lumborum occupies a large amount of space in the abdomen, it is near numerous structures. The intrinsic back muscles are dorsomedially placed, while the colon, kidneys, and diaphragm are ventrally positioned in relation to the muscle.
After leaving the lumbar plexus, the iliohypogastric and ilioinguinal nerves travel over the ventral aspect of the quadratus lumborum before continuing to the lateral abdominal muscles.
Embryology
The skeletal muscle is derived from the embryonic mesoderm leaflet, which is apparent as early as the second week of gestation.
In the medial-lateral direction, the mesoderm varies in four areas:
The notochord is composed of the chordomesoderm.
The paraxial mesoderm is divided into two slings: the longitudinal course and the lateral to the notochord. These slings are broken up into metameric tiny masses by the creation of transverse grooves.
The intermediate mesoderm in the cervical, thoracic, and caudal regions, next to the somites.
the lateral mesoderm that separated into two parallel sheets and was located farthest from the notochord.
The notochord, or initial axile apparatus of the embryo, is formed during embryonic development by the median cellular cord. It has a brief lifespan but is in charge of the induction phenomenon toward the surrounding regions. Beginning at the embryo’s cephalic end, the paraxial mesoderm (mesoderm on the sides of the notochord) is divided into two sets of cylindrical thickenings with a spiral organization known as somitomeres as a result of the creation of transverse grooves.
The most cranial portion of the mesoderm is when somitomere segmentation starts, with a more pronounced metamer in the cervical, thoracic, lumbar, sacral, and coccygeal areas.
The striated muscles of the face, jaw, and neck are formed by the first seven pairs of somitomeres, which have a little enhanced segmentation. These muscles are the next types of segmental units known as somites.
The first of the 42–44 somites that form corresponds to the eighth somitomere.
The occipital region is where the first four pairs of somites originate. Here, they aid in the development of the tongue, eye, and facial muscles in addition to the occipital and facial bones.
Following this, there are eight pairs of cervical somites: the first helps develop the occipital, while the other seven form the cervical vertebrae, muscles, and dermis.
Twelve pairs of thoracic somites form the vertebrae, musculature, and bones of the rib cage, and they enter the formation of the upper limb. Five pairs of lumbar somites form the lumbar vertebrae, muscles, and abdominal dermis. Five pairs of sacral somites form the sacrum and its corresponding muscles and dermis. Three to five pairs of coccygeal somites form the coccyx.
Clinical Importance
Symptom:
Lower back pain is often described as a deep aching pain. Walking, standing, and rolling over in bed may aggravate the pain.
Sharp pain may also be felt when sneezing or coughing. Quadratus lumborum pain can even interfere with doing everyday activities, such as walking and sitting.
Quadratus lumborum pain may also be chronic, which means it is long-lasting. Long-term pain often interferes with a person’s quality of life and well-being as well as affects them physically.
The QL may be involved in trigger points. This disorder could also resemble a lumbar pain syndrome.
The development of a heterotopic ossification, also known as myositis ossificans, is another cause of low back pain that is associated with the physical presence of QL. In the latter case, the etiopathogenesis may not always be evident or it may arise from direct damage and insufficient recovery.
It is important to remember that, aside from acute injuries, a single muscle rarely causes discomfort. The fascial system connects all of the muscles, and when one contractile area has changed function, it affects all of the surrounding muscular regions, making them all functionally challenging to use.
An excellent method for achieving non-surgical quality of life is through fascial osteopathic treatment. The latter is a more delicate process that honors the patient’s pain and helps them feel less discomfort.
According to a recent study, athletes with patellofemoral pain syndrome can experience pain relief and enhanced performance by using dry needling on the gluteus maximus and quadratus lumborum.
In 2007, Dr. Blanco Rafael became the first to do surgery under quadratus lumborum anesthesia. With the aid of ultrasound-guided assistance, both anterior and posterior access are legitimate lateral or intramuscular methods.
When anesthesia is given in this way, it covers dermatomes T4 to L2, travels through the paravertebral spaces and then disperses via blood, lymphatic, and nerve channels. This technique can be used to reduce pain after surgery (such as a gastrotomy, colostomy, cesarean section, laparoscopy, pyeloplasty, and more) as well as before surgery.
Surgery for Hip Fractures
Due to their advanced age and an increasing number of medical comorbidities, patients who appear with hip fractures are frequently clinically problematic. Thus, a primary objective of the overall care and management of these patients is the development of novel anesthetic procedures that, in an ideal world, balance the risk of anesthesia without sacrificing pain control.
For this particular patient group, the quadratus lumborum block (QLB) has shown clinical benefit in managing pain during surgery, either alone or in conjunction with other analgesic modalities.
11 Comments