
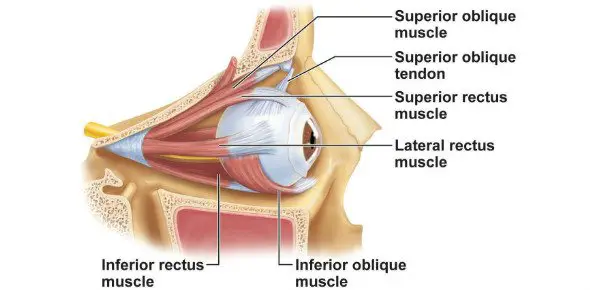
Inferior Oblique Muscle
Inferior oblique muscle is a thin, narrow muscle placed near the anterior margin of the floor of the orbit. It is one of six extraocular muscles that help to do eye movements.
Extraocular muscles are important for eye movement. The four rectus muscles, superior oblique, and inferior oblique muscles work together to move the eyes in various directions. The inferior oblique muscle is the main function of external rotation. The other actions are elevation and abduction.
Table of Contents
Anatomy
Origin:
orbital surface of the maxilla, lateral to the lacrimal groove .
Insertion:
laterally onto the eyeball, deep to the lateral rectus, by a short flat tendon.
The anterior edge of the orbital floor is in close proximity to the slender inferior oblique muscle. The inferior oblique muscle is not derived from the common tendinous ring (annulus of Zinn), in contrast to the superior oblique muscle and the recti muscles. Rather, the anterior aspect of the orbit is where the inferior oblique originates.
More specifically, from the nasolacrimal fossa directly lateral to the medial (orbital) surface of the maxilla. From there, it runs between the lateral rectus muscle and the orbital floor, ascending obliquely and posterolaterally. Posterior to the equator of the eyeball, the muscle inserts onto the inferolateral part of the sclera.
Blood supply and Lymphatics drainage:
the ophthalmic artery branches (a branch of the internal carotid artery), and a branch of the infraorbital artery.
Vein drains are The inferior orbital vein
Nerve supply:
oculomotor nerve (The inferior division of cranial nerve III).
Action:
extorsion, elevation, abduction.

The inferior oblique rotates the visual axis upward and outward by raising and abducting the eyeball. This is important because it involves movements of the eyes from a position of concentration, like looking up from reading.
Every extraocular muscle functions either cooperatively or antagonistically to one another. For instance, the superior rectus and inferior oblique muscles cooperate to raise the pupil, but their opposing rotatory movements also balance each other out.
It is crucial to use the complementary action to prevent the eyeball from rotating as it is being raised. Apart from its primary roles, the inferior oblique muscle collaborates with the check ligaments stated earlier and the retrobulbar fat to inhibit the rectus muscles from retracting the eyeball. The eyeball is supported by these structures, which also aid in maintaining its posture.
Relations
Between the lateral and inferior recti muscles, and slightly posterior to the insertion of the superior oblique muscle, the inferior oblique muscle attaches at the posterior quadrant of the eyeball (inferolateral portion). The inferior and superior oblique muscles lie in the same oblique vertical plane when their entering tendons pass one another.
The thicker sheath of the inferior rectus muscle melds with the inferior oblique’s fascial sheath. These two then merge with the triangular sheet expansions of the medial and lateral recti muscles, known as the medial and lateral check ligaments. The inferior rectus, inferior oblique, and check ligaments combine to form the suspensory ligament of the eyeball, which supports the eyeball like a hammock. Furthermore, an anterior expansion known as the inferior check ligament is released from the united sheaths of the inferior rectus and inferior oblique, and it attaches itself to the inferior eyelid’s tarsus.
Embryology
Prechordal mesoderm is the source of the inferior oblique, superior, inferior, and medial rectus muscles. Compared to the superior oblique, the inferior oblique is distinct in that it is virtually exclusively muscular as opposed to both muscular and tendinous.
Physiologic Variantions
Unusual variants of the extraocular muscles are uncommon but might include muscle duplication or absence, as well as abnormalities of the insertions or innervations. These differences may necessitate a surgical assessment since they can impair extraocular movement.
Clinical Significance
When inferior oblique dysfunction is diagnosed, parents and pediatricians can refer patients to an ophthalmologist early on. Patching the dominant eye can, in the early stages, compel the injured eye to strengthen and compensate. Later on, though, the patching method might not work, in which case surgical intervention is advised.
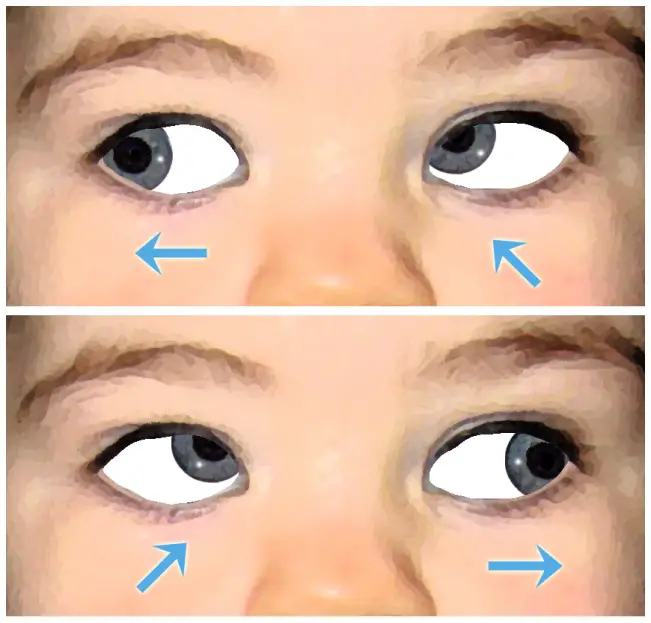
An damage to the inferior oblique muscle might occur during lower blepharoplasty excision. Individuals may exhibit symptoms that range from temporary diplopia to irreversible strabismus. When an inferior oblique injury causes diplopia, the condition typically manifests as distorted vision with upward lateral gaze. Patients frequently elevate their chins or tilt their heads inadvertently as a form of compensation.
Surgical Considerations
The eye is externally rotated, elevated, and abducted by the inferior oblique muscle. Any damage to this muscle can cause strabismus, an extraocular condition that can be easily noticed. Even if the patient might be able to compensate for their extraocular movement limitation, surgery is still necessary for cosmetic correction.
Thirty percent of exotropia patients and seventy percent of esotropia patients have inferior oblique overaction. A disproportionate elevation of the eye during an attempt at adduction is known as over-action.
There are two types of inferior oblique overaction: primary and secondary. Primary suggests that the patient had infantile esotropia due to bilateral inferior oblique overaction at birth. The second kind arises from a unilateral deficiency in the superior oblique muscle. The muscles involved in abduction, internal rotation, and depression are called superior oblique muscles. Because of this, the inferior oblique action is unopposed and causes severe elevation if the superior oblique muscle is paralyzed.
Recession, myectomy, extirpation and denervation, disinsertion, and anterior transposition of the muscle are surgical procedures used to treat inferior oblique overaction.
Patients with dissociated vertical deviation and inferior oblique overaction may benefit from the anterior transposition approach of the inferior oblique muscle.
The inferior oblique muscle becomes a depressor in this method. The muscle’s usual activity in the temporal 14 mm is greatly diminished. Upward gaze is restricted to 30 to 35 degrees due to the conversion of the posterior part of the inferior oblique into a depressor.
When a patient has dissociated vertical deviation but vertical hypertropia, a myectomy is performed. Retinal holes and tears are more common in patients with inferior oblique overaction. Therefore, a myectomy serves as a cosmetic repair as well as a preventive treatment. The muscle presses on the thin sclera in inferior oblique overaction, increasing the risk of a retinal tear or hole.
During enucleation, the transected inferior oblique muscle is frequently employed to give the globe traction.
FAQ
The eye is externally rotated, elevated, and abducted by the inferior oblique muscle. Any damage to this muscle can cause strabismus, an extraocular condition that can be easily noticed.
cranial nerve III
The inferior division of the oculomotor nerve (cranial nerve III) innervates the inferior oblique.
The inferior oblique muscle is located in the eye. It is one of the extraocular muscles responsible for controlling eye movements.
The inferior oblique muscle, like the other eye muscles, gets its name from where it resides in the orbit in relation to the eyeball. It surrounds the lower part of the eyeball and resides on the inferior face of the orbit. This muscle’s main function is to raise and abduct, or move, the eyeball laterally.
The infraorbital artery partially serves the inferior oblique and inferior rectus muscles, while the lacrimal artery partially supplies the lateral rectus muscle. The anterior ciliary arteries that accompany the rectus muscles are produced by the muscular branches; there are 1-4 anterior ciliary arteries for each rectus muscle.
The inferior oblique muscle can be tested by performing the “inferior oblique function test.” This involves asking the patient to look upward and inward while keeping the head straight. Dysfunction of the inferior oblique muscle may be indicated by limitations or abnormalities in these specific eye movements.
Excyclo and incyclotorsion are the principal activities of the inferior and superior obliques; elevation and depression are their secondary actions; and abduction is their tertiary action.
References
- Gupta, N. (2023, July 25). Anatomy, Head and Neck: Eye Inferior Oblique Muscles. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK545253/
- Sendić, G. (2023, October 30). Inferior oblique muscle. Kenhub. https://www.kenhub.com/en/library/anatomy/inferior-oblique-muscle


One Comment