
Sternocleidomastoid Muscle: Anatomy, Function, Exercise
Table of Contents
Sternocleidomastoid Muscle Anatomy
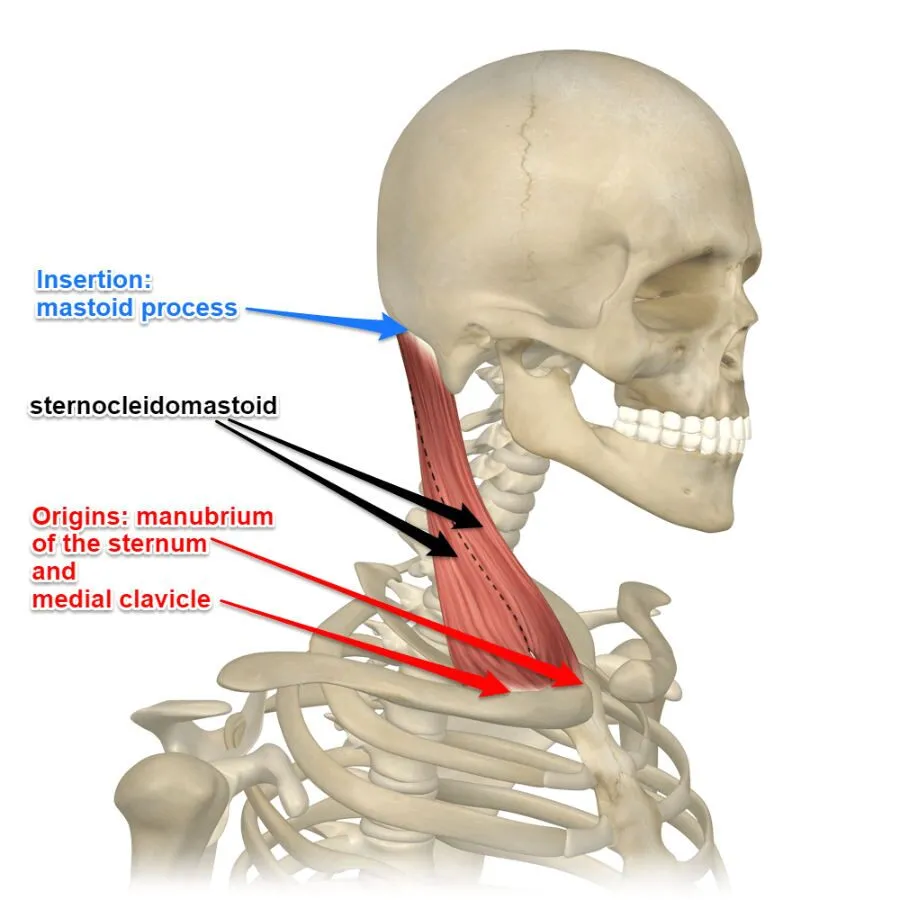
The sternocleidomastoid muscle is a two-headed long, bilateral muscle of the neck, and is the most visible cervical muscle. The main functions of the muscle are rotation of the neck to the opposite side and flexion of the neck. The muscle nerve supply is the accessory nerve.
The muscle name sternocleidomastoid is derived from the manubrium of the sternum (sterno-) and the clavicle (cleido-) and has an insertion at the mastoid process of the temporal bone of the skull.
Origin:
The muscles originate through two heads:
- Sternal head from superior part of anterior surface of manubrium sterni
- The clavicular head originates from the superior surface of the medial third of the clavicle
The sternal head originates from the anterolateral surface of the manubrium sterni while the clavicular head originates from the medial third of the superior surface of the clavicle, however, the thickness of the clavicular head is variable. These two heads are separated by a triangular surface depression known as a lesser supraclavicular fossa.
As muscle goes upwards, the clavicular head goes behind the sternal head and joins with its deep surface below the middle of the neck, forming a rounded thick belly.
Insertion:
Mastoid process of the temporal bone, superior nuchal line.
Nerve:
- Motor: spinal accessory nerve(11th cranial nerve).
- Sensory: sensory supply from C2 & C3
Blood Supply and Lymphatics
The occipital artery and superior thyroid artery, which are palpable with the pulse in the medial-anterior region of the muscle, are the branches of the external carotid artery that feed the SCM with blood. The blood flow to the respiratory muscles, including the SCM, rises during vigorous physical exercise, which is adverse to the limb muscles.
The external posterior and anterior jugular veins carry venous blood out of the body and empty it into the superior canal of the muscles (SCM).
The anterior superficial lymph nodes and the posterior triangle’s (inferior) lymph nodes make up the vertical chain of the neck’s lymphatic system, which drains the SCM.
Actions:


Unilaterally: contralateral cervical rotation, ipsilateral cervical flexion.
Bilaterally: cervical flexion, the elevation of the sternum, and assists in forced inhalation.
Accessory muscle for inspiration.
Relations
The muscle is visual and readily apparent since it is located quite superficially. The middle third of the front edge is where the carotid pulse may be felt. A neurovascular bundle that spans the sternocleidomastoid area contains the following:
- the medial common carotid artery
- the lateral internal jugular vein
- the dorsal vagus nerve
- Cervical ansa
A lead structure for the insertion of a central venous catheter (CVC) is the medial margin of the sternocleidomastoid muscle. The punctum nervosum, or Erb’s point, is where the dorsal branches of the cervical plexus meet with the muscle and can be punctured to administer local anesthetic.
Embryology
The SCM is largely derived from neural crests and comes from paraxial (pre-optic) mesoderm and occipital (post-optic) somites.
In animal models, the SCM emerges on the fourteenth day of gestation. A recent study found that within the cardiopharyngeal mesoderm, progenitor cells of the heart and the cells that will eventually create the neck’s muscles share space.
Physiologic Variants
Congenital agenesis of the SCM is an uncommon abnormality that may not result in any functional or clinical abnormalities. It may also entail the concurrent lack of trapezius muscle. This is most likely the result of other neck muscles making compensating adjustments.
The origin of the SCM is one of its other variants, and it might affect the outcome of a local surgical surgery. The clavicular attachment may impact the acromion-clavicular joint or exhibit many muscular bellies in the SCM. It may be small or large (up to about 7 to 8 cm) or have multiple clavicular attachments. It is recognized that insertions to the sternoclavicular joint alter the neck’s anatomical structure.
Unusually, there are more than one SCM muscle head. For instance, on one side, there are two sternomastoid, one cleido-occipital, and one cleidomastoid occipital origins; on the other, there is one sternomastoid, one cleido-occipital, and two cleidomastoid origins, totaling four muscle heads.
Occasionally, the SCM margin may come into direct touch with the trapezius, most often as a result of embryological defects. There exist varieties called cleido-epistrophic, cleido-cervical, and cleido-atlantic insertions, each with one or more heads.
The SCM’s innervation might differ. According to one research, the descendens hypoglossi, a branch of C1 from the ansa cervicalis, innervates the bottom section of the SCM; this is only possible for the upper portion of the muscle. The deep part of the top third of the SCM has been revealed to be innervated by an aberrant branch of the facial nerve.
The terms “nutator capitis,” “mastoideus colli,” “sternocleidomastoid muscle of Kopfnicker,” and “sternomastoid muscle” also denote the various forms of SCM.
With all of these anatomical factors in mind, proceed with caution while attempting surgery in this location.
Etymology
The reason it is called sternocleidomastoid is that it inserts at the mastoid process of the temporal bone of the skull, originating at the manubrium of the sternum (sterno-) and the clavicle (cleido-).
Sternocleidomastoid muscle exercise:
There are mainly two types of exercise: Stretching exercise and strengthening exercise.
Stretching exercise of the sternocleidomastoid muscle
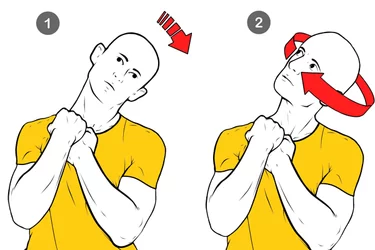
The Sternocleidomastoid Stretching exercise helps to improve the flexibility of the neck. It is one of the largest muscles of the neck. Tight SCM muscle makes the jaw protrude forward which may lead to heads out of its original position. Regular stretching exercise helps your muscles to relax and helps to normalize neck posture and overall the jaw can stay in its correct position.
How to stretch Sternocleidomastoid muscle?
To stretch SCM muscles, you should Sit on a chair with an upright posture.
Hold the chair with your right hand while your left hand supports the head.
Gradually bend your neck forward, then to the side bend to the left, and turn your head to the right.
Lean your body to the left and slightly forward.
Hold the stretch position for 10 to 20 seconds and relax.
Repeat the stretch on another side.
Strengthening exercise of Sternocleidomastoid muscle:
If you want to strengthen your patient’s left SCM muscles, you can use the right hand on the patient’s right face, command the patient to turn the head to the left side with try to push therapist’s hand, Hold for a few seconds and relax, Repeat 5 to 10 times and then also strengthen your sternocleidomastoid muscle.
Clinical importance:
Torticollis:
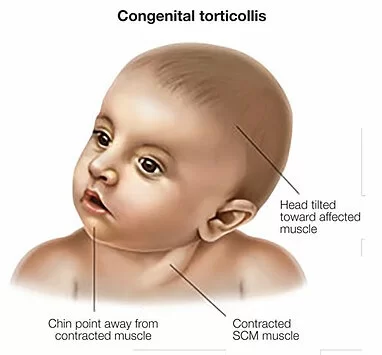
Torticollis is a condition that refers to a neck condition that causes the head to lean to one side. The muscles on one side are shorter than the other, causing the head to tilt towards the short muscles. There are many causes of torticollis, but the most common cause is an injury to the neck, usually from a car accident or another injury. Other causes include spasmodic torticollis or muscular dystrophy.
Physiotherapy Treatment
The consideration of both superficial and deep muscle layers is necessary for addressing SCM dysfunction.
Physiotherapy is crucial for treating congenital torticollis, which accounts for one-third of congenital muscle anomalies. It can also hasten healing following a potential surgical procedure. Stretching exercises, voluntary posture-improving motions (if the kid is not too tiny), or parent-made posture adjustments for the child are all examples of recommended conservative treatment. Thankfully, there is often a solution to the issue. Depending on the medical indication and the therapist’s assessment, several techniques to SCM may be used.
Intramuscular hemangioma, pseudosarcomatous proliferative myositis, pseudotumor of infancy (fibromatosis colli), and sternocleidomastoid rupture are among the disorders that may necessitate an initial surgical approach.
According to recent research, individuals with chronic neck pain exhibit more electrical activity in their SCM as compared to individuals without such discomfort. Individuals with persistent cervical discomfort exhibit a greater degree of fat infiltration in the SCM compared to those who do not experience pain.
For patients in this therapeutic setting, combining traditional physiotherapy with massage and stretching seems to be a beneficial approach.
Furthermore, changes in the SCM’s electromyographic spectrum are associated with temporomandibular diseases. This assessment method may be used to confirm the presence of mandibular dysfunctions.
Osteopathic treatment
Osteopathic therapy for SCM patients following surgery should have a beneficial effect on the production of scars. Osteopathic manipulation can treat the cervical myofascial layers as well as the gaps between the cervical vertebrae using mild, non-invasive procedures.
Sternocleidomastoid Muscle Assessment
In order to detect any hypotrophy of the sternocleidomastoid muscle (SCM) and postural anomalies of the neck and head, shoulder and scapula, clavicle, and sternal manubrium, the examination starts with the patient seated.
In order to assess motor or pain restrictions, the patient is asked to execute some voluntary neck movements. They are then asked to practice chewing and take a forced breath to see how the SCM responds.
A little tendon hammer is used to assess the reflexes at the SCM’s clavicular insertion. The patient moves their head in flexion, rotation, and inclination as the examiner applies little resistance to evaluate their level of muscular strength.
FAQ
The sternocleidomastoid (SCM) muscle is a strong neck muscle that enables you to tilt or rotate your head and bend your neck. Pain and stiffness may result from SCM injuries and stress. Osteopathic manipulation, physical therapy, and stretching are among the treatment methods.
Because it inserts at the mastoid process of the temporal bone of the skull and begins at the manubrium of the sternum (sterno-) and the clavicle (cleido-), it is known as the sternocleidomastoid.
The disorder known as muscular torticollis causes the sternocleidomastoid muscle on the affected side to shorten, which causes the face and chin to tilt ipsilateral and rotate contralaterally.
Acute or chronic neck stiffness with reduced mobility, particularly in rotation; may be accompanied with torticollis, nausea, tinnitus, vertigo, and neck discomfort as well as pain in body parts away from the neck (e.g., eyes, temples, throats, ears, nose, shoulders).
Accessory nerve
The cranial nerve that supplies the sternocleidomastoid and trapezius muscles is the accessory nerve, sometimes referred to as the eleventh cranial nerve, cranial nerve XI, or simply CN XI. Because part of it was thought to originate in the brain, it is ranked as the eleventh of the twelve pairs of cranial nerves.
One branch of the superior thyroid artery and the external carotid artery provide the majority of the blood flow for the middle part of the SCM muscle.
References
- Sternocleidomastoid muscle. (2023, June 12). In Wikipedia. https://en.wikipedia.org/wiki/Sternocleidomastoid_muscle
- Bordoni, B. (2023, April 4). Anatomy, Head and Neck, Sternocleidomastoid Muscle. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK532881/

12 Comments